
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 4(6); 2013 > Article
-
Original Article
In Vitro Antibacterial Efficacy of 21 Indian Timber-Yielding Plants Against Multidrug-Resistant Bacteria Causing Urinary Tract Infection - Monali P. Mishraa, Rabindra N. Padhyb
-
Osong Public Health and Research Perspectives 2013;4(6):347-357.
DOI: https://doi.org/10.1016/j.phrp.2013.10.007
Published online: November 7, 2013
aDepartment of Microbiology, IMS and Sum Hospital, Siksha ‘O’ Anusandhan University, Kalinga Nagar, Bhubaneswar 751003, Odisha, India
bCentral Research Laboratory, IMS and Sum Hospital, Siksha ‘O’ Anusandhan University, Kalinga Nagar, Bhubaneswar 751003, Odisha, India
- ∗Corresponding author. rnpadhy54@yahoo.com
© 2013 Published by Elsevier B.V. on behalf of Korea Centers for Disease Control and Prevention.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- To screen methanolic leaf extracts of 21 timber-yielding plants for antibacterial activity against nine species of uropathogenic bacteria isolated from clinical samples of a hospital (Enterococcus faecalis, Staphylococcus aureus, Acinetobacter baumannii, Citrobacter freundii, Enterobacter aerogenes, Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa).
-
Methods
- Bacterial strains were subjected to antibiotic sensitivity tests by the Kirby–Bauer's disc diffusion method. The antibacterial potentiality of leaf extracts was monitored by the agar-well diffusion method with multidrug-resistant (MDR) strains of nine uropathogens.
-
Results
- Two Gram-positive isolates, E. faecalis and S. aureus, were resistant to 14 of the 18 antibiotics used. Gram-negative isolates A. baumannii, C. freundii, E. aerogenes, E. coli, K. pneumoniae, P. mirabilis, and P. aeruginosa were resistant to 10, 12, 9, 11, 11, 10, and 11 antibiotics, respectively, of the 14 antibiotics used. Methanolic leaf extracts of Anogeissus acuminata had the maximum zone of inhibition size—29 mm against S. aureus and 28 mm against E. faecalis and P. aeruginosa. Cassia tora had 29 mm as the zone of inhibition size for E. faecalis, E. aerogenes, and P. aeruginosa. Based on the minimum inhibitory concentration and minimum bactericidal concentration values, the most effective 10 plants against uropathogens could be arranged in decreasing order as follows: C. tora > A. acuminata > Schleichera oleosa > Pterocarpus santalinus > Eugenia jambolana > Bridelia retusa > Mimusops elengi > Stereospermum kunthianum > Tectona grandis > Anthocephalus cadamba. The following eight plants had moderate control capacity: Artocarpus heterophyllus, Azadirachta indica, Dalbergia latifolia, Eucalyptus citriodora, Gmelina arborea, Pongamia pinnata, Pterocarpus marsupium, and Shorea robusta. E. coli, followed by A. baumannii, C. freundii, E. aerogenes, P. mirabilis, and P. aeruginosa were controlled by higher amounts/levels of leaf extracts. Phytochemicals of all plants were qualitatively estimated.
-
Conclusions
- A majority of timber-yielding plants studied had in vitro control capacity against MDR uropathogenic bacteria.
- A physician empirically treats acute infection ailment before prognostic evidence, such as antibiograms of causative bacteria, are available. However, a failure in the empiric therapy, because of the unknown mismatch of the prescribed antibiotic from the attack of multidrug-resistant (MDR) bacteria, would create a clinical mis-management that results in the progress of the ailment. If the infecting MDR bacterium is a balanced parasite, such as Pseudomonas or Staphylococcus or a few others, the bacterial progeny subtly migrates to various internal organs, following which pathogenicity progresses and the patient suffers from several comorbidities that could lead to septicemia/bacteremia. Further, the pathogen may spread in the community or in hospital settings during the progress of the disease, if it goes unchecked. Thus, the proper control of MDR pathogenic bacteria by an antimicrobial stewardship program remains an obvious uphill task. Whenever an MDR bacterial infection at innards of a patient even of a younger age remains intractable, it slowly results in a terminal complicated illness. Subsequently, the patient may be transferred from the intensive care unit (ICU) to a hospice. By contrast, if the invasive MDR bacterium is a destructive parasite, such as Vibrio or Salmonella or Diplococcus, an acute life-threatening situation would occur rapidly. To treat patients in both types of situations, a combination therapy with ongoing antibiotics is often followed, which however, has its intrinsic limitations of mild to acute side effects, as exemplified by tubercle bacillus chemotherapy [1]. Consequently, the physician has a dilemma as to whether to use a higher generation antibiotic or not.
- Originally inhabiting the nasal nares and other soft tissues of the body, the commensal organism Staphylococcus aureus has become resistant to the β-lactam group of antibiotics. The subsequently emerged strain—methicillin-resistant S. aureus (MRSA) has become even more MDR, with 95% resistance to antibiotics in use nowadays [2]. Those with further resistance to the most preferred antibiotic vancomycin (vancomycin-resistant S. aureus or VRSA) could now be called MDR–MRSA–VRSA strains, which are regarded as the superbugs of the health domain [2]. In addition, MDR bacterial strains originate independently everywhere as complex nexuses and occur far and wide from the place of origin, including its insidious spread in communities. In parallel, among Gram negatives (GNs), Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa have developed strains that are resistant to almost all antibiotics available today and are informally called pandrug-resistant bacteria. Most GN bacteria, with a remarkable capacity of survival and dissemination, dispel the “clean” idea of the ICU of a hospital [3]. Their MDR strains are normally intractable in any infection episode, including urinary tract infections (UTIs), suppurating wounds, or bloodstream infections, etc., thereby causing a fear of the onset of various ailments in people of all age groups. For example, a metallo-β-lactamase strain of K. pneumoniae was responsible for the death of a neonate from acute septicemia in our hospital recently [4]. Not surprisingly, among infectious diseases, UTI is the second most common ailment, next to infections of the chest/lungs, in causing mortality [5].
- Further, the precipitation of numerous public health episodes is linked to one or other MDR bacterial strain at each geographical zone or country [6–8]. For example, the Gram-positive (GP) enteropathogen Clostridium difficile with unmatchable notoriety had precipitated two public health episodes in North India alone [9,10]. Similarly, in rural Odisha, MDR Vibrio cholerae precipitated several sporadic episodes of short durations in Aborigine societies in the last decade, causing mortality in men, women, and children [11]. Further, our school has pursued studies on surveillance of common pathogenic bacteria, such as P. aeruginosa [3], S. aureus [2], Escherichia coli [12], as well as the less common strains of Staphylococci and Enterococci from community and hospital sectors [13], the results of which indicated the high levels of multidrug resistance in each pathogen. In addition, studies on systematic surveillance of enteropathogens [11] and uropathogens [14,15] gave pictures of the rapid infection dynamics of two classes of pathogens recently, in addition to explaining the distress experienced by aged, critical, and immunocompromised patients.
- Indeed, any or several species of the nine bacteria causing UTIs more frequently infect females (i.e., more than 50% of the population), as reported in our earlier surveillance of hospital sectors [15]. UTIs can cause cystitis, pyelonephritis, and prostatitis, leading to bacteremia/septicemia at an organ, depending on the invasive nature of the pathogen, which enters the bloodstream through the kidneys; such infections often cause terminal illness with multiple comorbidities, subsequently leading to fatality [16]. Obviously, a noncommittal attitude on the issue of diseases caused by multiple infections with MDR bacteria by the clinician, due to the lack of a suitable control agent, would be a medical infraction. Thus, these peripatetic pathogens need be controlled. Thus, complementary, supplementary or alternative therapies are also sought. Plants always remain a tangible source of nonmicrobial antimicrobials [17].
- In the crusade against MDR pathogens, a herbaceous terrestrial fern (Lygodium flexuosum) was reported to have promising control effects on both MDR enteropathogens and uropathogens [18]. Being encouraged by the novelty in the use of crude phytoextracts, several higher plants were also used for monitoring the in vitro control efficacy against MDR pathogenic bacteria by our school [19–21]. Indeed, higher plant extracts with an array of phytocompounds were never overcome by any pathogenic bacteria, no matter how MDR they were [17]. Continuing this line of work, several important mostly nonedible timber-yielding plants were chosen from our subtropical forest, to evaluate their antimicrobial efficacy against MDR UTI-causing bacteria, which are documented here. In general, timber-yielding plants live long and have huge stem growth with darkened heart wood in the central zone, which is laden with an array of secondary metabolites, rendering the wood stronger and termite resistant; in addition, these metabolites are present in considerable quantities in barks and leaves as well [22]. Obviously, the characteristic feature of timber-yielding plants is their more unique secondary metabolites, capable of evading the wood-destroying pests which is superior to that of herbs or trees that do not yield quality timber [23]. Moreover, a noncommittal attitude on phytocompounds is nowadays regarded as the pejorative disposition of the natural wealth of drugs, in an era in which plant products for use in complementary and alternative medicine (CAM) are gaining in popularity, even in developed countries [24–26], with the obvious tenet of comparing their success against controls.
- Previously reported bacterial uropathogens isolated from clinical samples [15] were used in this study for monitoring the in vitro antimicrobial activity with methanol extracts of 21 timber-yielding plants. We chose to extract, isolate, and characterize the pure antimicrobials only from the leaves of the chosen plants, as choosing to extract the antimicrobials from the bark/heartwood results in heavy damage to plants, especially when large amounts of these alternative sources are used for developing CAM in the future. For the control of the uropathogens, there is a logistic need to prepare a formulation of coalesced effective phytochemicals as CAM along with mainstream medicine in empiric therapy. Because these formulations are obtained eukaryotic sources, the bacterial armamentaria would be ineffective to cause any resistance against these CAMs. Obviously, the host toxicity testing of phytodrugs is an essential corollary in drug development. The great number of phytocompounds stands is a potential unending source of drugs, promising a potential business of plant-based drugs for general well-being and control of many diseases [26]. It is anticipated that the areas of pharmacognosy, pharmacology, and pharmaceutics could take up the work on isolation and characterization of pure phytocompounds of effective plants and their standardization as antimicrobials, because bacterial genomes are changing rapidly or rather dramatically to win over newer antibiotics, which create the fear of precipitation of future public health episodes.
Introduction
- 2.1 Collection of plants and preparation of extracts
- The plants used in this study were collected from the Kandha tribe, who inhabit the hills in the Eastern range of mountains of India, in the district of Kalahandi (Odisha, India), in February 2013. A total of 70 respondents of 25 hamlets were interviewed in a forest patch and the recorded information was documented (Table 1). The snowball method of survey and sampling was used, as previously followed [27]. The collected dried leaf samples were crushed to powder form; 10 g of powder from a sample was dissolved in an aliquot of 100 mL of methanol and incubated at 4 °C for 72 hours and the suspension was filtered. The methanolic filtrate was concentrated in a rotary evaporator at 40 °C, until a sticky mass was obtained that was weighed and dissolved in an aliquot of 1.0 mL of 10% vol/vol dimethyl sulfoxide (DMSO). The mass was stored at 4 °C until further use.
- 2.2 Isolation, identification of bacterial strains, and antibiotic sensitivity test
- Two GP bacteria, S. aureus and Enterococcus faecalis, and seven GN bacteria, A. baumannii, Citrobacter freundii, Enterobacter aerogenes, E. coli, K. pneumoniae, Proteus mirabilis, and P. aeruginosa, were used in the study. All these bacteria were directly collected from clinical samples of Sum Hospital, Bhubaneswar (Odisha, India) using an appropriate medium, specific for the respective bacterium [15]. All bacterial strains were subjected to antibiotic sensitivity tests by the Kirby–Bauer's disc diffusion method, using a 4-mm thick Mueller–Hinton (MH) agar (HiMedia, Mumbai, India) medium, following the standard antibiotic susceptibility test chart of the Clinical Laboratory Standard Institute guidelines, as described previously [3,15].
- 2.3 Antibacterial test of plant extracts
- The agar-well diffusion method was used for monitoring the antibacterial potentiality of plant extracts with gentamicin 30 mg/mL as the standard, and one strain from each bacterial species showing resistance to a maximum number of antibiotics was used for analysis [18,20]. Antibacterial activities were evaluated by measuring the diameter values of zones of inhibition; the monitoring experiment of each solvent extract was conducted three times and results of the third repetition are presented. It was confirmed that 10% DMSO had no inhibitory effect on any bacterium.
- 2.4 Determinations of minimum inhibitory concentration and minimum bactericidal concentration of plant extracts
- Minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) of the active plant extracts were determined. Original stock solutions of leaf extracts were prepared with methanol, using 100 mg plant extract/mL of 10% DMSO solution, and distilled with water. Each stock solution was diluted to obtain final concentrations of 0, 1.562, 3.125, 6.25, 12.5, 25, 50, and 100 mg/mL with the DMSO solution. A separate experiment was conducted for each plant extract. An aliquot of 80 μL of each dilution of a plant extract was released into a well on a 96-well (12 × 8) microtiter plate, along with an aliquot of 100-μL MH broth, an aliquot of 20-μL bacterial inocula (109 colony forming units/mL), and a 5-μL aliquot of 0.5% 2,3,5-triphenyltetrazolium chloride (TTC). After pouring all the aforementioned ingredients into a well, the microplate was incubated at 37 °C for 18 hours. The development of pink coloration due to TTC indicated bacterial growth, whereas the absence of the color indicated inhibition of bacterial growth. The first well of the microplate was the control without any plant extract. The MIC value was noted at the well where no color appeared. Further, bacteria from each well of the microplate were subcultured on a nutrient agar plate; the level of dilution, where no bacterial growth on the nutrient agar plate was observed, was noted as the MBC value [20].
- 2.5 Qualitative phytochemical analyses
- The following tests were performed for the plant species used: reducing sugars, anthraquinones, saponins, flavonoids, steroids/terpenes, tannins, alkaloids, resins, and glycosides, as detailed previously [18,19,21].
Materials and methods
- The ethnomedicinal information on 21 timber-yielding plants is documented along with details of modalities of crude extracts used as medicine for many ailments by local ethnic Aborigine groups (Table 1). It is discernible from the recorded information that most plants are in use for cough, diarrhea, diabetes, bronchitis, fever/ pyrexia, killing worms, constipation, heart problems; thus, the majority of plant parts are edible as medicines. In addition, the fruits of Artocarpus heterophyllus, Bridelia retusa, Eugenia jambolana, and Mimusops elengi are also edible.
- The antibiotic profile of each pathogenic bacterium was determined using specified antibiotic discs (Table 2). The GP isolates, E. faecalis and S. aureus, were resistant to 14 of the 18 antibiotics used. Among the seven GN isolates, A. baumannii, C. freundii, E. aerogenes, E. coli, K. pneumoniae, P. mirabilis, and P. aeruginosa were resistant to 10, 12, 9, 11, 11, 10, and 11 antibiotics, respectively, of the total 14 antibiotics used. The antibiotic susceptibility results of the isolated bacteria are provided in Table 2. Thus, all isolated bacterial strains were MDR.
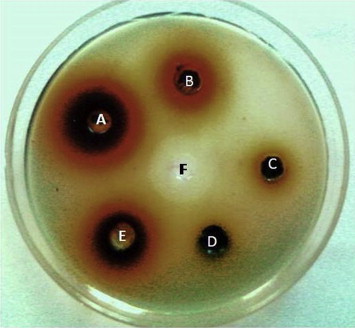
- Methanolic extracts of 21 plants were tested against nine MDR bacterial species for antibacterial properties by the agar-well diffusion method and the values of zone of inhibition were recorded (Table 3). The methanolic extracts of Anogeissus acuminata had a zone of inhibition size of 29 mm against S. aureus and 28 mm against both E. faecalis and P. aeruginosa (Figure 1). Thus, the most effective 12 plants at least causing a zone of inhibition 25–29 mm (for both GP and GN MDR strains used) were A. acuminata, Anthocephalus cadamba, Azadirachta indica, B. retusa, Cassia tora, Eucalyptus citriodora, E. jambolana, Pterocarpus santalinus, Schleichera oleosa, Shorea robusta, Stereospermum kunthianum, and Tectona grandis. The unique 10 plants (from 21 plants) that controlled all the pathogens were A. acuminata, A. cadamba, B. retusa, C. tora, E. jambolana, M. elengi, P. santalinus, S. oleosa, S. kunthianum, and T. grandis, and some of these were without the highest value of 29 mm as the zone of inhibition size. Moderate control capacity was exhibited by the following eight plants (from 21 plants): A. heterophyllus, A. indica, Dalbergia latifolia, E. citriodora, Gmelina arborea, Pongamia pinnata, Pterocarpus marsupium, and S. robusta. The remaining three plants (from 21 plants), Albizia lebbeck, Alstonia scholaris, and Melia azedarach, had the least control over all these MDR bacteria. Detailed data regarding the zones of inhibition by the 21 methanolic plant extracts were recorded (Table 3).
- The MDR strains of E. faecalis, S. aureus, A. baumannii, and P. aeruginosa were controlled by extracts of all plants. C. freundii was not controlled by only A. lebbeck; E. aerogenes was not controlled by A. scholaris, G. arborea, M. azedarach, and S. robusta; E. coli was not controlled by A. lebbeck, A. scholaris, A. heterophyllus, M. azedarach, and P. pinnata; K. pneumoniae was not controlled by D. latifolia, E. citriodora, M. azedarach, P. pinnata; and P. mirabilis was not controlled by A. heterophyllus, A. indica, G. arborea, and P. marsupium.
- The MIC and MBC values of methanolic extracts of timber-yielding plants were evaluated. A. acuminata had 0.67 mg/mL as the lowest MIC value and 1.51 mg/mL as the lowest MBC value against E. faecalis and S. aureus, but had the highest MIC value of 9.63 mg/mL and the highest MBC value of 21.67 mg/mL for E. coli. A lower MIC/MBC value signifies that a minimum amount (lower level) of plant extract was used, whereas a higher value signifies using a larger amount of plant extract for the control of any bacterium. Based on MIC and MBC values, effective plants could be arranged in the following order (decreasing): C. tora > A. acuminata > S. oleosa > P. santalinus > E. jambolana > B. retusa > M. elengi > S. kunthianum > T. grandis > A. cadamba. E. coli, followed by A. baumannii, C. freundii, E. aerogenes, P. mirabilis, and P. aeruginosa were controlled by higher amounts/levels of leaf extracts, as evident from the MIC and MBC values. The MIC and MBC values of all bacteria are presented in Tables 4–6.
- Qualitative phytochemical analysis was performed for these plants. A. acuminata, B. retusa, C. tora, E. citriodora, E. jambolana, P. santalinus, S. kunthianum, S. oleosa contained the many phytochemicals, including alkaloids, flavonoids, carbohydrates, terpenoids, steroids, tannins, resins, saponins, and anthraquinones, which explains the recorded significant antibacterial activities. Plants of less control capacity, namely, A. lebbeck, A. scholaris, and M. azedarach, as well as the moderately effective ones, D. latifolia, P. pinnata, and P. marsupium, contained limited phytochemicals. The result of phytochemical analysis of all these plants was recorded (Table 7).
Results
- This work demonstrated that methanolic extracts of 10 plants, C. tora, A. acuminata, S. oleosa, P. santalinus, E. jambolana, B. retusa, M. elengi, S. kunthianum, T. grandis, and A. cadamba in the order of effectivity as stated, were the most effective against the nine isolated MDR uropathogens.
- The MDR bacteria could be considered as the return of an enemy with extra strength (i.e., with multiple antibiotic resistance), after being partially injured by an antibiotic that would eliminate all sensitive strains; however, one or more drug-resistant cell(s) survived. Further, defenses produced by the host body are sometimes counteracted by the drug resistance of invading pathogens, as successful parasites live to reproduce, and the pathogenesis is the result. Moreover, many obvious factors trigger their emergence: first, a latest generation antibiotic for the control of an infection is empirically used; and the antibiotic used empirically may be changed after the antibiotic sensitivity report of the sample arrives; second, sometime the history of antibiotics used previously by the patient during is unknown or not taken in account; third, irregularity in the intake of antibiotics by the patient in the treatment period; fourth, intake of medicines without a prescription by patients, seen in some countries (e.g., Japan); fifth, based on symptoms of upper respiratory tract infections, a physician might prescribes antibiotics without confirming the causative agent, which may turn out to be a viral infection; and last, the infrequent application of combination therapy with two or more antibiotics at a relatively lower dose of each, to avoid the nontarget host toxicity. These issues individually may appear less prominent or trivial, but their cumulative effects can cause independent emergences of MDR pathogens everywhere [3].
- Several timber-yielding plants reported here were used for several ailments by ethnic groups and their medicinal effects were studied by various groups from other parts of India. For example, P. pinnata was used traditionally by ethnic people for the treatment of bronchitis, whooping cough, rheumatic joint pain, and to quench dipsia in diabetics [28]. The watery extract of P. marsupium is known for the treatment of diabetes due to the presence of pterostilbene [29]. Stereospermum personatum had been reported to have antibacterial, antifungal, and hypoglycemic activity against p338 lymphocytic leukemia [30]. Ethyl ether and alcoholic leaf extracts of A. lebbeck had successfully controlled standard strains of S. aureus and E. coli that infected Wistar rats without any acute toxicity up to levels of 200–400 mg/kg of the extract [31]. Ethanolic extracts of A. lebbeck pods are known to possess antiprotozoal, anticancer, and hypoglycemic properties. Species of Acacia and Albizia controlled drug-sensitive strains of E. coli, Klebsiella sp., and P. aeruginosa; however, the extracts from these plants could not control the GP Bacillus subtilis [32]. The ocular pathogenic bacterium Corynebacterium macginleyi was controlled by methanolic extracts from several trees [33]. Methanolic extracts of Terminalia catappa, Terminalia chebula, Rosa indica, A. lebbeck, and Butea monosperma had been reported to have the maximum antibacterial activity; among the 40 plants studied, 90% plants had antibacterial activity [33]. The antibacterial activity of M. azedarach extracts in solvents such as methanol, ethanol, petroleum ether, and water against standard strains of Bacillus cereus, S. aureus, P. aeruginosa, E. coli, and many fungi had been recorded previously [34]. Five organic solvents and water extracts of A. scholaris had been shown to have the control over three GP organisms, including S. aureus and five GN organisms, including E. coli, P. aeruginosa, and P. mirabilis [35]. The MIC values were determined with lipophilic and aqueous leaf extracts against four GP bacteria, namely, B. cereus, Streptococcus mutans, Lactobacillus acidophilus, and S. aureus, two GN bacteria, namely, E. coli and K. pneumoniae and two yeasts, namely, Candida albicans and Cryptococcus neoformans. Moderate to high antimicrobial activity of Sida cuneifolia against several uropathogens were recorded with MIC values ranging from 0.4 to 6.0 mg/mL [36].
- The most popular herbal medicines used by Aborigines do not have institutional/scientific/clinical/pharmaceutical validation and host toxicity testing for the direct use as drugs in mainstream medicine. Many of the concoctions of crude phytodrugs among the cited plants are used as preventives for many diseases, but their curative roles are mostly not established. By contrast, several reports of plants have documented host toxicity in humans [37]. The antioxidant and hepatoprotective activity of the timber-yielding plant Soymida febrifuga was recorded previously [38]. The methanolic and aqueous extracts of this plant had been shown to have considerable phenolic contents. Furthermore, crude extracts from S. kunthianum were shown to exert hypotensive and/or hypoglycemic activities on rats [39].
- Located at the eastern range of mountains in the state, with a 40% Aborigine population, the Kalahandi district is richer in vegetation in comparison with other hilly patches of the state. These Aborigine people pass their ethnomedicinal knowledge orally in a secretive manner down through the generations. Furthermore, India with tropical and subtropical forest areas is a home to approximately 550 million plants that serve as the source of traditional medicine (TM), derived from the clandestine ethnic information and Ayurveda [40]. In TM, plants are used in several ways and they are popular for several concoctions and specific modalities for many crucial and common diseases, which have facilitated modern drug development and the use of finished herbal medicines as different formulations, in the herbal medicine trade [26]. TM as a field remains as the major accessible and affordable method of treatment for marginalized urban people and Aborigines. Indeed, TM has been in use in several developed Western countries, as an important mode of CAM [41,42]. According to a previous report, 48% of the population in Australia, 70% in Canada, 42% in the United States, 38% in Belgium, and 75% in France use CAM [43]. Such crude phytodrugs are available in market shelves everywhere and many people like to depend on them, for their well-being or health-boosting effects. For example, Artemisia annua has been in use in China for malaria originally and its active ingredient (i.e., artemisinin) is now used along with mefloquine in mainstream medicine as CAM for malaria [44], so as to overcome the problem of drug resistance.
- Large proportions of plant drugs are popular for their performance standards, and are in general use. Here two examples are the use of the decoction of internodes of the antidiabetic Tinospora cordifolia in India and Panax ginseng (ginseng) root, which is best known to lower blood sugar and cholesterol levels, protect against stress, enhance strength, and promote relaxation, from the Eastern world with a remarkable popularity in the United States. Many health-boosting formulations, concocted with many herbal products, have been gaining popularity in Brazilian, American, and Chinese societies [45], and that is also occurring in equal or lesser dimensions in many other countries. Several of these products have some planned clinical evaluations of treatment modality, therapy, and in the marketing of patented formulations [46]. Moreover, several pharmaceutical companies are busy worldwide in preparing and marketing several combinations of natural products as medicines for different purposes, parallel to the scientific exactitude of drug preparations and uses, systematically followed in mainstream medicine [45]. Planned commercial medicinal plant growing establishments are slowly developing in several states in India, apart from government-approved collections of plants of interest from forests [27].
- It is possible that when other organic solvents could be used alternately with these 21 plants, a more varied picture of the level of control might be obtained. However, methanol is routinely used as a solvent in the protocol of bioassay-guided fractionation of crude phytoextracts, because of its capability to extract polar, moderately polar, and nonpolar compounds from crude extracts holistically—a characteristic which is not present in most other organic solvents, and is a basic requirement for the isolation of active phytocompounds of specific interest.
- In conclusion, the data embodied here demonstrate that MDR UTI bacteria could be well-controlled in vitro, using crude methanolic leaf extracts of the 18 timber-yielding plants described. A total of 10 plants were selected in this study and were shown to have effective control against bacteria, and these could be further studied for isolation and purification of pure phytocompounds and their host toxicity. Thus, those could further be incorporated into CAM as empiric therapies, to prevent the untoward devastation which may be caused by MDR bacteria.
Discussion
-
Acknowledgements
- This work is a part of PhD thesis of M.P.M. in Biotechnology (Siksha ‘O’ Anusandhan University). This work, as well as M.P.M. as a JRF, is supported by the major research project on “Development of standardized herbal extracts against urinary tract bacterial inflection. (Grant No. BT/PR8214/PBD/17/863/2013), from the Department of Biotechnology, Government of India, New Delhi (India). We are thankful to IMS and Sum Hospital for extended facilities and Sri G. Kar, Managing Member, IMS and Sum Hospital for encouragements.
Acknowledgments
-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article information
- 1. Dubey D., Rath S., Sahu M.C.. Status of multidrug resistance in tubercle bacillus and phytochemicals for the control. J Public Health 21(1). 2013 Feb;115−119.Article
- 2. Dubey D., Rath S., Sahu M.C.. Surveillance of infection status of drug resistant Staphylococcus aureus in an Indian teaching hospital. Asian Pac J Trop Dis 3(2). 2013 Apr;133−142.Article
- 3. Sahu M.C., Rath S., Dubey D.. Multidrug resistance of Pseudomonas aeruginosa as known from surveillance of nosocomial and community infections in an Indian teaching hospital. J Public Health 20(4). 2012 Jan;413−423.Article
- 4. Dubey D., Sarangi R., Debata N.K., Padhy R.N.. Detection of metallo-β-lactamase producing Klebsiella pneumoniae in a neonatal septicemia. J Acute Dis 2(1). 2013 Mar;82−84.Article
- 5. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 171(4). 2005 Feb;388−416. PMID: 15699079.ArticlePubMed
- 6. Quintero B., Araque M., van der Gaast-de Jongh C.. Epidemiology of Streptococcus pneumoniae and Staphylococcus aureus colonization in healthy Venezuelan children. Eur J Clin Microbiol Infect Dis 30(1). 2011 Jan;7−19. PMID: 20803226.ArticlePubMed
- 7. Sengstock D.M., Thyagarajan R., Apalara J.. Multidrug-resistant Acinetobacter baumannii: an emerging pathogen among older adults in community hospitals and nursing homes. Clin Infect Dis 50(12). 2010 May;1611−1616. PMID: 20462357.ArticlePubMed
- 8. Yu F., Fan S., Fan X.. Analysis of characteristics of paratyphoid A in 157 Chinese inpatients between 1998 and 2009. Eur J Clin Microbiol Infect Dis 30(1). 2011 Jan;71−75. PMID: 20827496.ArticlePubMed
- 9. Rani P., Khullar N.. Antimicrobial evaluation of some medicinal plants for their anti-enteric potential against multidrug resistant Salmonella typhi. Phytother Res 18(8). 2004 Aug;670−673. PMID: 15476301.ArticlePubMed
- 10. Vaishnavi C., Singh M.. Preliminary investigation of environmental prevalence of Clostridium difficile affecting inpatients in a north Indian hospital. Indian J Med Microbiol 30(1). 2012 Jan–Mar;89−92. PMID: 22361768.ArticlePubMed
- 11. Rath S., Padhy R.N.. Surveillance of multidrug resistance of 10 enteropathogens in a teaching hospital and in vitro efficacy of 25 ethnomedicinal plants used by an Indian aborigine. Asian Pac J Trop Dis 2(1). 2012 Oct;S336−S346.Article
- 12. Rath S., Dubey D., Sahu M.C.. Surveillance of ESBL producing multidrug resistant Escherichia coli in a teaching hospital in India. Asian Pac J Trop Dis 4(2). 2014 Apr;140−149.Article
- 13. Dubey D., Padhy R.N.. Surveillance of multidrug resistance of two Gram-positive pathogenic bacteria in a teaching hospital and in vitro efficacy of 30 ethnomedicinal plants used by an aborigine of India. Asian Pac J Trop Dis 2(4). 2012 Aug;273−281.Article
- 14. Rath S., Dubey D., Sahu M.C.. Surveillance of multidrug resistance of 6 uropathogens in a teaching hospital and in vitro control by 25 ethnomedicinal plants used by an aborigine of India. Asian Pac J Trop Biomed 2(2). 2012 Aug;S818−S829.Article
- 15. Mishra M.P., Debata N.K., Padhy R.N.. Surveillance of multidrug resistant uropathogenic bacteria in hospitalized patients—an Indian study. Asian Pac J Trop Biomed 3(4). 2013 Apr;315−324. PMID: 23620859.ArticlePubMed
- 16. Giamarellos-Bourboulis E.J., Papadimitriou E., Galanakis N.. Multidrug resistance to antimicrobials as a predominant factor influencing patient survival. Int J Antimicrob Agents 27(6). 2006 Jun;476−481. PMID: 16707252.ArticlePubMed
- 17. Sahu M.C., Dubey D., Rath S.. In vitro efficacy of 30 ethnomedicinal plants used by an Indian aborigine against 23 multidrug resistant pathogenic bacteria. J Herb Med 2013;in press.
- 18. Nayak N., Rath S.N., Mishra M.P.. Antibacterial activity of the terrestrial fern Lygodium flexuosum (L.) Sw. against multidrug resistant enteric- and uro-pathogenic bacteria. J Acute Dis 2(4). 2013 Dec;270−276.Article
- 19. Dubey D., Padhy R.N.. Antibacterial activity of Lantana camara L. against multidrug resistant pathogens from ICU patients of a teaching hospital. J Herb Med 3(2). 2013 Jun;65−75.Article
- 20. Rath S., Padhy R.N.. Monitoring in vitro antibacterial efficacy of Terminalia alata Heyne ex. Roth, against MDR enteropathogenic bacteria isolated from clinical samples. J Acute Med 3(3). 2013 Sep;93−102.Article
- 21. Sahu M.C., Padhy R.N.. In vitro efficacy of Butea monosperma Lam. against 12 clinically isolated multidrug resistant bacteria. Asian Pac J Trop Dis 3(3). 2013 Jun;217−226.
- 22. Nuopponen M.H., Birch G.M., Sykes R.J.. Estimation of wood density and chemical composition by means of diffuse reflectance mid-infrared Fourier transform (DRIFT-MIR) spectroscopy. J Agric Food Chem 54(1). 2006 Jan;34−40. PMID: 16390174.ArticlePubMed
- 23. Ali M.. Pharmacognosy (pharmacognosy and phytochemistry). vol. 1:2011. CBS Publishers and Distributors; New Delhi: p 802.
- 24. WHO. Global atlas of traditional, complementary and alternative medicine. 2005. World Health Organization; Geneva.
- 25. MacLennan E., Pendry B.A.. The evolution of herbal medicine as an unorthodox branch of British medicine: the role of English legislation from antiquity to 1914. J Herb Med 1(1). 2011 Sep;2−14.Article
- 26. Dubey D., Rath S., Sahu M.C.. Antimicrobials of plant origin against multi-drug resistant bacteria including the TB bacterium and economics of plant-drugs—Introspection. Indian J Tradit Knowl 11(2). 2012 Apr;225−233.
- 27. Mallik B.K., Panda T., Padhy R.N.. Traditional herbal practices by the ethnic people of Kalahandi district of Odisha, India. Asian Pac J Trop Biomed 2:2012;S988−S994.Article
- 28. Kirtikar K.R., Basu B.D.. 2nd ed.Indian medicinal plants. vol. 1:1995. International Book Distributors; Dehradun.
- 29. Subbarao A.V.. The chemistry of natural products—three decades in Andhra Pradesh, India. 1975. Andhra Pradesh Academy of Sciences; Visakhapatnam: p 214.
- 30. Bakuni D.S., Dhar M.L., Dhar M.M.. Screening of Indian plants for biological activity: III. Indian J Exp Biol 9(1). 1971 Jan;91−102. PMID: 5089325.PubMed
- 31. Chulet R., Jhajharia M., Pradhan P., Sharma S.. Analgesic and antipyretic activity of Albizzia lebbeck. Pharmacology online 3:2010;737−749.
- 32. Mahmood A., Mahmood A., Qureshi R.A.. Antimicrobial activities of three species of family mimosaceae. Pak J Pharm Sci 25(1). 2012 Jan;203−206. PMID: 22186331.PubMed
- 33. Koday N.K., Rangaiah G.S., Bobbarala V.. Bactericidal activities of different medicinal plants extracts against ocular pathogen viz Corynebacterium macginleyi. Drug Invent Today 2(1). 2010 Jan;5.
- 34. Sen A., Batra A.. Evaluation of antimicrobial activity of different solvent extracts of medicinal plant: Melia azedarach L. Int J Curr Pharm Res 4(2). 2012 Mar;67−73.
- 35. James J., Veettil A.K.T., Kumar P.. Phytochemical investigation and antibacterial activity of the fruits of Alstonia scholaris. Int J Phytopharmacol 3(1). 2012;74−77.
- 36. van Vuuren S.F., Viljoen A.M.. The in vitro antimicrobial activity of toothbrush sticks used in Ethiopia. S Afr J Bot 72(4). 2006 Nov;646−648.Article
- 37. Bussmann R.W., Malca G., Glenn A.. Toxicity of medicinal plants used in traditional medicine in Northern Peru. J Ethnopharmacol 137(1). 2011 Sep;121−140. PMID: 21575699.ArticlePubMed
- 38. Reddy B.S., Reddy R.K., Reddy B.P.. Potential in vitro antioxidant and protective effects of Soymida febrifuga on ethanol induced oxidative damage in HepG2 cells. Food Chem Toxicol 46(11). 2008 Nov;3429−3442. PMID: 18812207.ArticlePubMed
- 39. Kodjo K.M., Contesse V., Do Rego J.L.. In vitro effects of crude extracts of Parkia biglobosa (Mimosaceae), Stereospermum kunthianum (Bignoniaceae) and Biophytum petersianum (Oxalidaceae) on corticosteroid secretion in rat. J Steroid Biochem Mol Biol. 100(4–5). 2006 Aug;202−208. PMID: 16820293.ArticlePubMed
- 40. Desilva T., Bahorun T., Sahu M., Le Mai H.. Traditional and alternative medicines, research and policy perspectives. 2009. Daya Publishing House; New Delhi.
- 41. Lee J., Bielory L.. Complementary and alternative interventions in atopic dermatitis. Immunol Allergy Clin North Am 30(3). 2010 Aug;411−424. PMID: 20670822.ArticlePubMed
- 42. Pineda M.J., Singh D.K.. What is integrative oncology and can it help my patients? Obstet Gynecol Clin North Am 39(2). 2012 Jun;285−312. PMID: 22640716.ArticlePubMed
- 43. WHO. World Health Organization traditional medicine strategy 2011 [Internet]. 2011. World Health Organization; Geneva: pp 1−14. Available from,. http://apps.who.int/medicinedocs/documents. [accessed 15.10.13].
- 44. Bloland P.B., Ettling M., Meek S.. Combination therapy for malaria in Africa: hype or hope? Bull World Health Organ 78(12). 2000;1378−1388. PMID: 11196485.PubMedPMC
- 45. Lam K.S.. New aspects of natural products in drug discovery. Trends Microbiol 15(6). 2007 Jun;279−289. PMID: 17433686.ArticlePubMed
- 46. Gautam R., Saklani A., Jachak S.M.. Indian medicinal plants as a source of antimycobacterial agents. J Ethnopharmacol 110(2). 2007 Mar;200−234. PMID: 17276637.ArticlePubMed
References
| Serial No. | Plant name | Family | Local name | Parts used | Ethnomedicinal uses |
|---|---|---|---|---|---|
| 1 | Albizia lebbeck (L.) Benth. | Fabaceae | Sirisha | Leaf/bark | Used to treat cough, boil, stomach problems. Bark is used to treat inflammations. |
| 2 | Alstonia scholaris L.R.Br | Apocynaceae | Chhatiana | Bark | Bark is used for malaria, diarrhea, snake bite, urinary tract, and skin problems. |
| 3 | Anogeissus acuminata (Roxb. ex DC.) Wall. ex Guill. & Perr | Combretaceae | Phasi | Leaf/bark | Its leaf has wound-healing activity, and is used in inflammation, and skin diseases. Its bark is used to treat diabetes. |
| 4 | Anthocephalus cadamba (Roxb.) Miq. | Rubiaceae | Kadamba | Leaf/bark | Its bark is used for urinary infections. Leaf is used to cure diarrhea, fever, inflammation, cough, vomiting, and wounds. |
| 5a | Artocarpus heterophyllus Lam. | Moraceae | Panasa | Leaf | The leaves are useful in fever, boils, wounds, skin diseases. The leaf ash, with corn and coconut shells, is used alone or mixed with coconut oil to heal ulcers. |
| 6 | Azadirachta indica L. Adelb. | Meliaceae | Nimb | Leaf | Used as an antiseptic as it has antibacterial and antiviral action (chicken pox). It is used for the treatment of acne. |
| 7a | Bridelia retusa (L.) Spreng. | Euphorbiaceae | Kasi | Bark | The bark is used against urinary tract problems. |
| 8 | Cassia tora L. | Leguminosae | Chakunda | Leaf, seed | The leaves and seeds are useful in treating leprosy, ringworm, constipation, cough, bronchitis, heart problems. |
| 9 | Dalbergia latifolia Roxb. | Fabaceae | Sisu | Bark | Bark is used for diarrhea, leprosy, and worms. |
| 10 | Eucalyptus citriodora Hook. | Myrtaceae | Nilagiri | Leaf | Leaf is used to cure fever, cold, wounds, skin ailments, and diabetes. |
| 11a | Eugenia jambolana Lam. | Myrtaceae | Jamu | Seed | Seed is used for treatment of diabetes. It is also used for ulcers. |
| 12 | Gmelina arborea Roxb. | Verbenaceae | Gambhari | Root | Root is used for burning sensations, fever, piles, and urinary discharges. |
| 13 | Melia azedarach L. | Meliaceae | Mahanimb | Leaf | Fresh leaf extract is used to cure burns, inflammation of the gum, pyrexia. |
| 14a | Mimusops elengi L. | Sapotaceae | Baula | Leaf/bark | Its bark and leaf extracts are used for urinary tract infections, diarrhea, wound, headache, dental problems, and constipation. |
| 15 | Pongamia pinnata L. | Leguminosae | Karanja | Leaf/root | Leaf juice aids in treatment of leprosy, gonorrhea, diarrhea, coughs, and cold. Root is used as a toothbrush and for killing worms. |
| 16 | Pterocarpus marsupium Roxb. | Fabaceae | Piasala | Bark | Paste of the bark of the plant with the barks of Mangifera indica, Shorea robusta, and Spondias pinnata is used to treat loose motion. |
| 17 | Pterocarpus santalinus Linn.f. | Fabaceae | Rakta-chandan | Leaf/bark | Used as an antiseptic, wound-healing agent, and in antiacne treatment. |
| 18 | Schleichera oleosa (Lour.) Oken | Sapindaceae | Kusuma | Seed | Seed oil is used for massage in rheumatism. |
| 19 | Shorea robusta Roth. | Dipterocarpaceae | Sala | Leaf | Used for wound healing and diarrhea; leaf powder with honey will help in improving blood purification. |
| 20 | Stereospermum kunthianum Cham. | Bignoniaceae | Padala | Leaf/bark | Leaf is used to treat sexual diseases and leprosy. Stem bark is used to cure loose motion, bronchitis, cough, fever, and arthritis. |
| 21 | Tectona grandis L. | Lamiaceae | Saguan | Bark | Used as an antiseptic, wound-healing agent, and in antiacne treatment. |
Antibiotics used: μg/disc.
Ac = amikacin 30; Ak = amoxiclav 30; Am = ampicillin 10; Cd = clindamycin 2; Ce = ceftriaxone 30; Cf = cefpodoxime 10; Ch = chloramphenicol 30; Cot = co-trimoxazole 25; Ge = gentamicin 10; Gt = gatifloxacin 5; Le = levofloxacin 5; Lz = linezolid 30; MS = moderately sensitive; ND = not done; Nx = norfloxacin 10; Of = ofloxacin 5; Ox = oxacillin 1; Pt = piperacillin/tazobactam 100/10; R = resistant; S = sensitive; Tei = teicoplanin 5; Va = vancomycin 30.
Numbers 1–21 are serial numbers of plants given in Table 1; values are measurements of zone of inhibition due to methanol extracts. The “—” sign denotes no activity.
Numbers 1–7 are serial numbers of plants given in Table 1; values are measurements of MIC and MBC due to methanolic extracts. The “—” sign denotes no activity. MIC = minimum inhibitory concentration; MBC = minimum bactericidal concentration.
Numbers 8–14 are serial numbers of plants given in Table 1; values are measurements of MIC and MBC due to methanolic extracts. The “—” sign denotes no activity. MIC = minimum inhibitory concentration; MBC = minimum bactericidal concentration.
Numbers 15–21 are serial numbers of plants given in Table 1; values are measurements of MIC and MBC due to methanolic extracts. The “—” sign denotes no activity. MIC = minimum inhibitory concentration; MBC = minimum bactericidal concentration.
Figure & Data
References
Citations
- Chemical constituents, pharmacological activities, and uses of common ayurvedic medicinal plants: a future source of new drugs
Parul Kaushik, Priyanka Ahlawat, Kuldeep Singh, Raman Singh
Advances in Traditional Medicine.2023; 23(3): 673. CrossRef - Antibacterial activity of Libyan Juniperus phoenicea L. leaves extracts against common nosocomial pathogens
Aml O. Alhadad, Galal S. Salem, Suliman M. Hussein, Sarah M. Elshareef
Journal of Experimental Biology and Agricultural S.2023; 11(2): 371. CrossRef - The Ethnopharmacology, Phytochemistry and Bioactivities of the Corymbia Genus (Myrtaceae)
Matthew J. Perry, Phurpa Wangchuk
Plants.2023; 12(21): 3686. CrossRef - Gas Chromatography-Mass Spectroscopic, high performance liquid chromatographic and In-silico characterization of antimicrobial and antioxidant constituents of Rhus longipes(Engl)
Adedoyin Adetutu Olasunkanmi, Olumide Samuel Fadahunsi, Peter Ifeoluwa Adegbola
Arabian Journal of Chemistry.2022; 15(2): 103601. CrossRef - Evaluation of the sensory attributes of pepper soup beef hides and determination of the preservative potential of the spices used for its preparation
T.C.L. Maguipa, P.D. Mbougueng, H.M. Womeni
Journal of Agriculture and Food Research.2022; 8: 100293. CrossRef - Flourensia retinophylla: An outstanding plant from northern Mexico with antibacterial activity
D. Jasso de Rodríguez, M.C. Victorino-Jasso, N.E. Rocha-Guzmán, M.R. Moreno-Jiménez, L. Díaz-Jiménez, R. Rodríguez-García, J.Á. Villarreal-Quintanilla, F.M. Peña-Ramos, D.A. Carrillo-Lomelí, Z.A. Genisheva, M.L. Flores-López
Industrial Crops and Products.2022; 185: 115120. CrossRef - Antibacterial Screening, Biochemometric and Bioautographic Evaluation of the Non-Volatile Bioactive Components of Three Indigenous South African Salvia Species
Margaux Lim Ah Tock, Sandra Combrinck, Guy Kamatou, Weiyang Chen, Sandy Van Vuuren, Alvaro Viljoen
Antibiotics.2022; 11(7): 901. CrossRef - Computational in Silico Modelling of Phytochemicals as a Potential Cure
Rachita Kurmi, Kavya N R, Jennath Sherin A, Silpa T S
International Journal of Scientific Research in Sc.2021; : 42. CrossRef - Hepatoprotective effects of Cassiae Semen on mice with non-alcoholic fatty liver disease based on gut microbiota
Hanyan Luo, Hongwei Wu, Lixia Wang, Shuiming Xiao, Yaqi Lu, Cong Liu, Xiankuo Yu, Xiao Zhang, Zhuju Wang, Liying Tang
Communications Biology.2021;[Epub] CrossRef - Phytochemical screening, anthocyanins and antimicrobial activities in some berries fruits
Amina A. Aly, Hoda G. M. Ali, Noha E. R. Eliwa
Journal of Food Measurement and Characterization.2019; 13(2): 911. CrossRef - Antimicrobial activity of select edible plants from Odisha, India against food-borne pathogens
Sujogya Kumar Panda, Yugal Kishore Mohanta, Laxmipriya Padhi, Walter Luyten
LWT.2019; 113: 108246. CrossRef - Extracts of Tectona grandis and Vernonia amygdalina have anti-Toxoplasma and pro-inflammatory properties in vitro
Mlatovi Dégbé, Françoise Debierre-Grockiego, Amivi Tété-Bénissan, Héloïse Débare, Kodjo Aklikokou, Isabelle Dimier-Poisson, Messanvi Gbeassor
Parasite.2018; 25: 11. CrossRef - Psacalium paucicapitatum has in vitro antibacterial activity
D. Jasso de Rodríguez, L.C. García-Hernández, N.E. Rocha-Guzmán, M.R. Moreno-Jiménez, R. Rodríguez-García, M.L.V. Díaz-Jiménez, A. Sáenz-Galindo, J.A. Villarreal-Quintanilla, F.M. Peña-Ramos, M.L. Flores-López, D.A. Carrillo-Lomelí
Industrial Crops and Products.2017; 107: 489. CrossRef - Qualitative Phytochemical Analysis, Antimicrobial Activity and Cytotoxic Effect of Moringa concanensis Nimmo Leaves
Ramaswamy Malathi, Solaimuthu Chandrasek
Research Journal of Medicinal Plants.2017; 11(3): 93. CrossRef - In vitro antibacterial activity of crude extracts of 9 selected medicinal plants against UTI causing MDR bacteria
Monali P. Mishra, Sibanarayan Rath, Shasank S. Swain, Goutam Ghosh, Debajyoti Das, Rabindra N. Padhy
Journal of King Saud University - Science.2017; 29(1): 84. CrossRef - Phytochemical investigation and antimicrobial assessment of Bellis sylvestris leaves
Monica Scognamiglio, Elisabetta Buommino, Lorena Coretti, Vittoria Graziani, Rosita Russo, Pina Caputo, Giovanna Donnarumma, Brigida D⿿Abrosca, Antonio Fiorentino
Phytochemistry Letters.2016; 17: 6. CrossRef - The genus Anogeissus: A review on ethnopharmacology, phytochemistry and pharmacology
Deeksha Singh, Uttam Singh Baghel, Anshoo Gautam, Dheeraj Singh Baghel, Divya Yadav, Jai Malik, Rakesh Yadav
Journal of Ethnopharmacology.2016; 194: 30. CrossRef - Antibacterial activity of five Peruvian medicinal plants against Pseudomonas aeruginosa
Gabriela Ulloa-Urizar, Miguel Angel Aguilar-Luis, María del Carmen De Lama-Odría, José Camarena-Lizarzaburu, Juana del Valle Mendoza
Asian Pacific Journal of Tropical Biomedicine.2015; 5(11): 928. CrossRef - In vitro antibacterial efficacy of plants used by an Indian aboriginal tribe against pathogenic bacteria isolated from clinical samples
Shasank S. Swain, Rabindra N. Padhy
Journal of Taibah University Medical Sciences.2015; 10(4): 379. CrossRef - Monitoring in vitro antibacterial efficacy of 26 Indian spices against multidrug resistant urinary tract infecting bacteria
Sibanarayan Rath, Rabindra N. Padhy
Integrative Medicine Research.2014; 3(3): 133. CrossRef
 PubReader
PubReader Cite
Cite
