Associations of pre-existing cardiovascular morbidity with severity and the fatality rate in COVID-19 patients: a systematic review and meta-analysis
Article information

Abstract
Objectives
The aim of this study was to evaluate the association of pre-existing cardiovascular comorbidities, including hypertension and coronary heart disease, with coronavirus disease 2019 (COVID-19) severity and mortality.
Methods
PubMed, ScienceDirect, and Scopus were searched between January 1, 2020, and July 18, 2020, to identify eligible studies. Random-effect models were used to estimate the pooled event rates of pre-existing cardiovascular disease comorbidities and odds ratio (OR) with 95% confidence intervals (95% CIs) of disease severity and mortality associated with the exposures of interest.
Results
A total of 34 studies involving 19,156 patients with COVID-19 infection met the inclusion criteria. The prevalence of pre-existing cardiovascular disease in the included studies was 14.0%. Pre-existing cardiovascular disease in COVID-19 patients was associated with severe outcomes (OR, 4.1; 95% CI, 2.9 to 5.7) and mortality (OR, 6.1; 95% CI, 2.9 to 12.7). Hypertension and coronary heart disease increased the risk of severe outcomes by 3 times (OR, 3.2; 95% CI, 2.0 to 3.6) and 2.5 times (OR, 2.5; 95% CI, 1.7 to 3.8), respectively. No significant publication bias was indicated.
Conclusion
COVID-19 patients with pre-existing cardiovascular comorbidities have a higher risk of severe outcomes and mortality. Awareness of pre-existing cardiovascular comorbidity is important for the early management of COVID-19.

Introduction
The ongoing coronavirus disease 2019 (COVID-19) pandemic poses a significant public health threat to all nations worldwide [1,2]. As of August 23, 2021, COVID-19 has infected approximately 212,763,099 people, including roughly 4,447,912 patients who have died. Regrettably, these numbers have kept increasing worldwide, indicating that the peak is far from over and the global community remains on edge as the number of infected patients continues to escalate.
Several studies from different countries have reported that pre-existing cardiovascular comorbidities are prevalent among COVID-19 patients [3−6]. Understanding the association of cardiovascular comorbidities with the severity and outcomes of COVID-19 may highlight a cohort of patients who require more intensive monitoring during the early phase of infection [7,8]. Epidemiological studies have reported different mortality rates for COVID-19 patients with cardiac manifestations and pre-existing cardiovascular diseases, particularly hypertension and coronary artery disease [8].
Several studies have investigated the association between pre-existing cardiac disease and COVID-19 severity and fatality, and the pooled effects have been estimated in a number of meta-analyses. However, previous reviews varied in how COVID-19 severity was defined; did not report the country of the studies, and reported substantial heterogeneity. Therefore, the present meta-analysis was performed with the following aims: (1) to estimate the overall prevalence rate of pre-existing cardiovascular disease and cardiac manifestations in COVID-19 patients, and (2) to evaluate the association of pre-existing hypertension and coronary heart disease with the severity of COVID-19 and the mortality rate in COVID-19 patients using a random-effect model that incorporates heterogeneity.
Materials and Methods
Data Search
Three databases (PubMed, Science Direct, and Scopus) were searched between January 1, 2020, and July 18, 2020. The following combined keywords were used for searching the databases: cardiovascular and COVID-19; cardiovascular and severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2); cardiovascular, and SARS-CoV-2; cardiovascular, hypertension, and COVID-19. Furthermore, the lists of references of all relevant studies were also manually checked to identify further studies. The protocol for this meta-analysis is registered at PROSPERO CRD42020191768. The meta-analysis was reported following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement [9].
Study Selection
The study selection was limited to articles in English and studies on adult humans. Case reports, review articles, and editorials were excluded from this analysis. Studies were selected if they provided adequate details on pre-existing cardiovascular disease comorbidities, particularly in patients with positive diagnoses for COVID-19 and hypertension. Studies that did not provide enough details on the number of cases with severe or fatal outcomes were excluded.
Data Abstraction
For studies that met the inclusion criteria, the following data were extracted from each study using a standardized form: the surname of the first author; the design of the study; ratios of clinical characteristics of interest; sample size, country, data relevant to cardiovascular disease comorbidities factor; and pertinent data for arrhythmia and acute cardiac injury as outcomes, and the number of cases with severe and non-severe outcomes, and the number of survivors and non-survivors. As reported in the included studies, severe disease was identified if patients needed to be admitted to the intensive care unit, needed vital life support, or required mechanical ventilation. Non-survivors were defined as cases of death. Two investigators (FA and MA) extracted the relevant data.
Quality Assessment
We used the Joanna Briggs Institute (JBI) critical appraisal checklist for case series to assess the risk of bias [10]. The JBI includes 10 items dealing with confounding, selection, and information bias to assess the internal validity of the case series. The answers for each of the 10 items in the JBI checklist could be “yes,” “no,” “unclear,” or “not applicable.” A detailed description of how to use the JBI tool is provided by Munn et al. in 2020 [10]. It is advised that the results of the quality assessment of the included studies should not be shortened and reported as a score [10]. The quality assessment of the included studies in this meta-analysis was carried out by SA.
Quantitative Data Synthesis and Analysis
Data analysis was carried out using Comprehensive Meta-Analysis V2 (Biostat, Englewood, NJ, USA). A p-value of <0.05 was considered statistically significant. Random-effect models were used to estimate the pooled event rates of pre-existing cardiovascular disease comorbidities as well as the odds ratio (OR) with 95% confidence intervals (95% CIs) of disease severity and mortality associated with the exposures of interest. A random-effect model was used to incorporate heterogeneity among studies [11]. Heterogeneity in any analysis was tested by using the I2 statistic (p<0.1), which estimates the percentage of variation in study results that is explained by between-study heterogeneity rather than sampling error. Usually, an I2 value >50% indicates considerable heterogeneity [11]. Funnel plots and Egger test were used to assess the presence of publication bias.
Results
Search Results and Study Characteristics
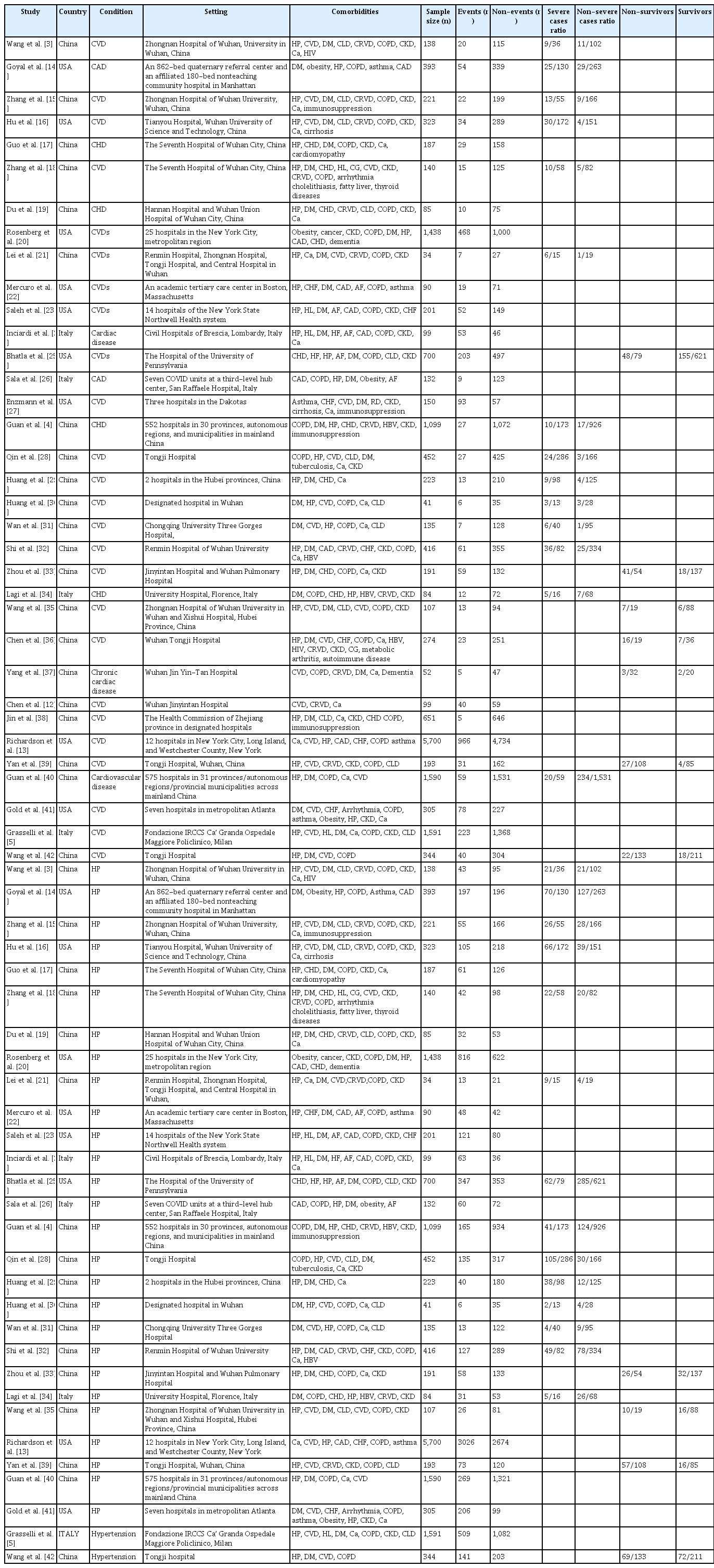
A total of 1,601 articles were identified from the 3 databases examined and other sources. After excluding duplicated or overlapping articles and removing reviews and editorials, 169 articles met the primary search criteria. For the quantitative part of our study, 34 studies that reported the event rate of pre-existing cardiovascular disease, arrhythmia, or acute cardiac injury as disease complications were included in the meta-analysis (Figure 1). Most studies were conducted in China (n=21) and the United States of America (n=8), while 4 studies were conducted in Italy and 1 study reported results from different parts of the world. The setting for most of the included studies was the hospital (Table 1) [3−5,12−42].

Flow chart of the literature search and study selection.
Number of patients with CVD comorbidities among coronavirus disease 2019 patients
Quantitative Analysis
The proportions of cardiovascular disease comorbidities and cardiac manifestations in COVID-19 patients
Relevant data regarding the event rate of pre-existing cardiovascular diseases, including hypertension and coronary heart disease, in 19,156 patients with COVID-19 were collected from 34 studies (Table 1) [3−5,12−42]. The pooled prevalence of pre-existing cardiovascular diseases or coronary heart disease among the included studies was 14% (95% CI, 11% to 17%), as is shown in Figure 2.
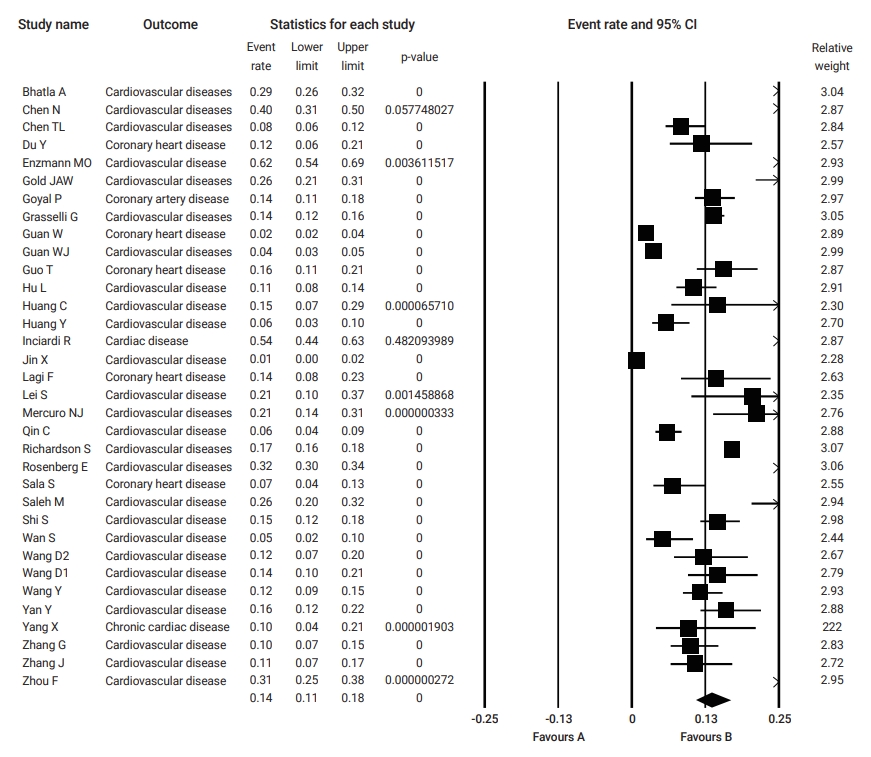
Pooled event rate of pre-existing cardiovascular disease in patients with coronavirus disease 2019. CI, confidence interval.
Pre-existing cardiovascular disease, hypertension, and coronary heart disease and the risk of severity outcomes and mortality in COVID-19
Table 2 summarizes the results of the current analysis. COVID-19 patients with pre-existing cardiovascular comorbidities were 4 times more likely to have severe outcomes (OR, 4.1; 95% CI, 2.9 to 5.7) (Figure 3) or not survive the disease (OR, 6.1; 95% CI; 2.9 to 12.7) (Figure 4), compared to patients with no pre-existing cardiovascular or coronary heart diseases. Severe disease was defined as patients needing to be admitted to the intensive care unit, needing vital life support, or requiring mechanical ventilation. Hypertension as a comorbid factor was associated with 2.6 times higher risk for severe outcomes (OR, 2.6; 95% CI, 1.9 to 3.6) and a 3 times higher fatality rate (OR, 3.2; 95% CI, 2.0 to 5.0) (Figures 5 and 6). However, coronary heart disease was associated with a 2.5 times higher risk for severe outcomes (OR, 2.5; 95% CI, 1.7 to 3.8) (Figure 7).

Effect of cardiovascular comorbidities on severity and mortality outcomes associated with coronavirus disease 2019
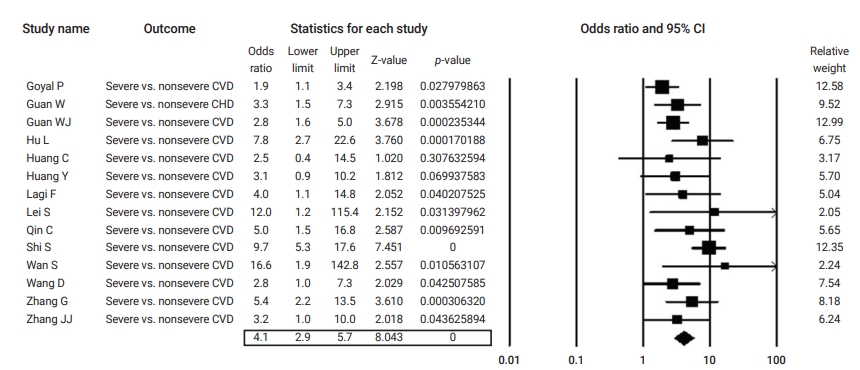
Forest plot of the odds ratios of pre-existing cardiovascular disease (CVD) in severe cases compared to non-severe cases of coronavirus disease 2019.
CI, confidence interval; CHD, coronary heart disease.

Forest plot of the odds ratios of pre-existing cardiovascular disease (CVD) in non-survivor compared to survivor coronavirus disease 2019 patients. CI, confidence interval.
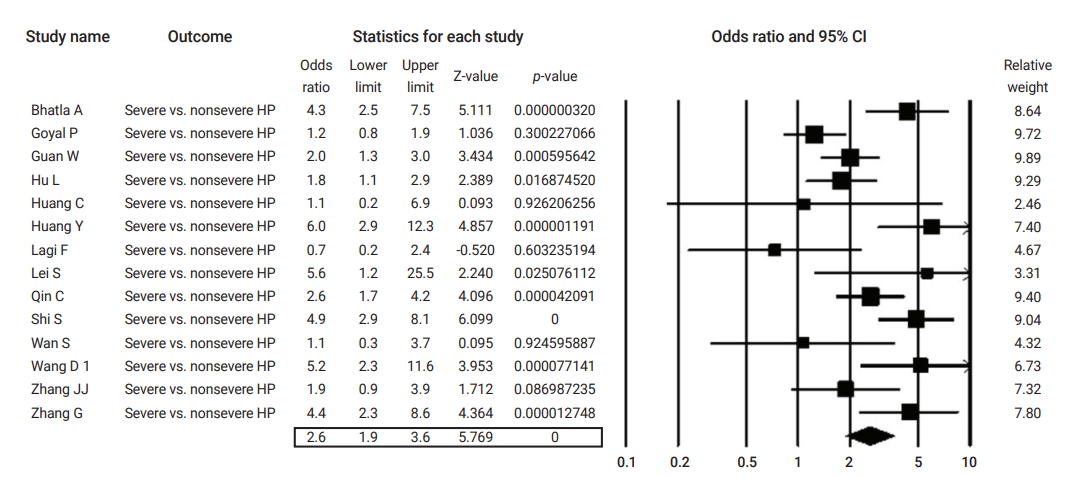
Forest plot of the odds ratios of pre-existing hypertension (HP) in severe compared to non-severe coronavirus disease 2019 cases. CI, confidence interval.
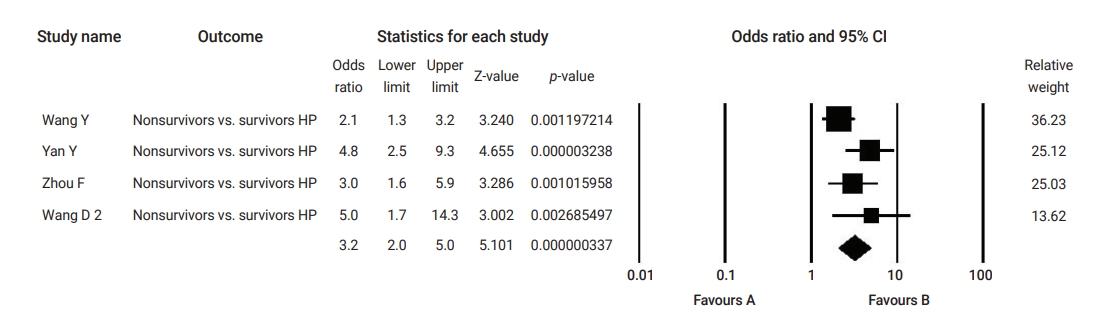
Forest plot of the odds ratios of pre-existing hypertension (HP) non-survivor compared to survivor coronavirus disease 2019 patients. CI, confidence interval.
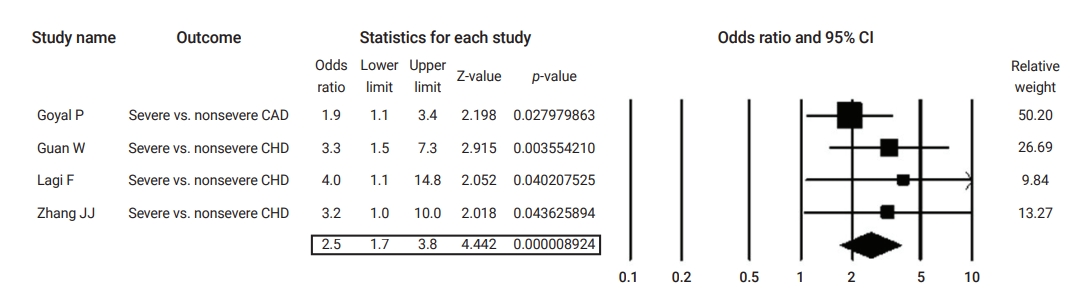
Forest plot of the odds ratios of pre-existing coronary heart disease (CHD) in severe cases compared to non-severe coronavirus disease 2019 cases.
CAD, coronary artery disease; CI, confidence interval.
Quality of the Included Studies
Table S1 shows the quality assessment of the studies on cardiovascular disease as a comorbidity in COVID-19 patients using JBI’s tool [3−5,12−42]. Most of the studies did not define participants’ eligibility criteria. Moreover, most studies were unclear regarding whether they included consecutive participants and whether the inclusion was complete. The majority of the studies diagnosed COVID-19 and the outcomes of interest using valid and reliable methods. All included studies in this analysis reported the demographic and the clinical characteristics, as well as the outcomes of the participants. However, most of the multi-center studies did not present the demographic and the clinical characteristics by site or clinic.
Assessment of Publication Bias
Publication bias was evaluated visually using a funnel plot. As shown in Figure 8 on the event rate of pre-existing cardiovascular comorbidity, a visual symmetry indicates the absence of publication bias. The Egger test also revealed no significant publication bias (Egger test, p=0.09).
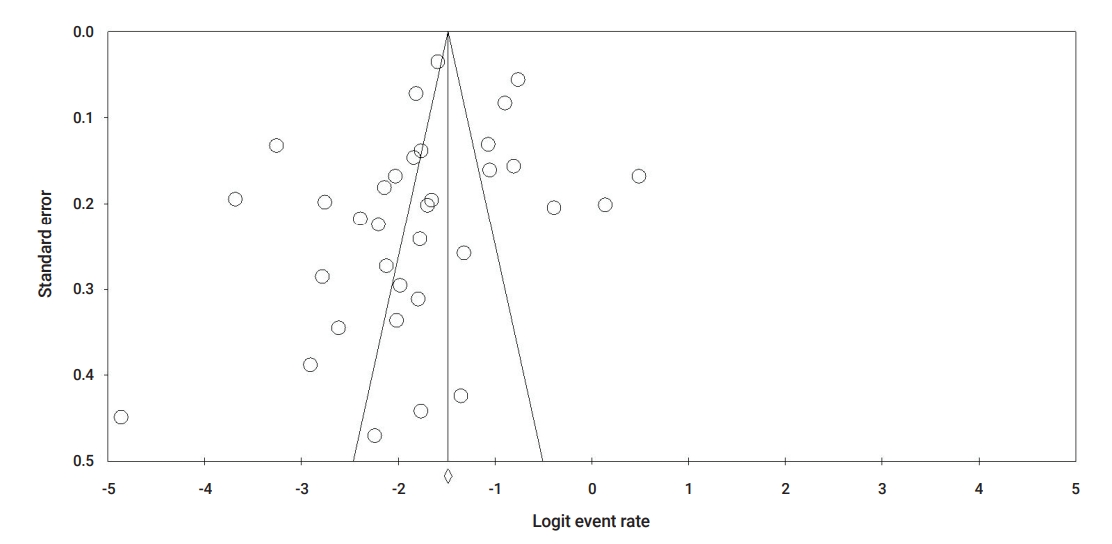
Funnel plot for publication bias based on cardiovascular comorbidity.
Discussion
In the present meta-analysis, we examined 36 independent studies reporting clinical data on 19,156 patients with COVID-19 worldwide. The studies included in this meta-analysis include the latest research available on COVID-19 from January to July 2020. Our pooled analyses indicated that pre-existing cardiovascular diseases, in particular hypertension and coronary heart disease, are prevalent among patients with COVID-19. Our pooled analyses also clearly showed that the presence of pre-existing cardiovascular disease, including hypertension and coronary heart disease, is associated with COVID-19 severity and/or fatality. This association can be confounded by older age, patients with poor outcomes may be older and have more cardiovascular events [43]. In this analysis meta-regression (data are not shown) using the method of moments of the effect of age, reported as mean or median, on association of pre-existing cardiovascular disease with COVID-19 outcomes revealed that age was significantly associated only with estimated OR for severity in patients with pre-existing cardiovascular disease.
In comparison, another meta-analysis of 6 published studies from China including 1,527 patients with COVID-19 that reported a 16.4% prevalence of cardio-cerebrovascular disease [44]. Another analysis of 7 Chinese studies showed that the prevalence of cardiovascular disease and that of hypertension were 21% and 8%, respectively [45]. Our meta-analysis on data from different countries reported a 14% prevalence of cardiovascular disease.
Pre-existing cardiovascular disease was associated with a 4-fold and 6-fold greater risk of disease severity and fatality, respectively. A previous study that analysed data of COVID-19 patients until March 20, 2020 found that cardiovascular disease increased the odds of combined critical/fatal cases of COVID-19 by 5 times [46] and in particular, hypertension was found to increase the odds of combined critical and fatal cases by 2.7 times. The main difference between our analysis and that by Zheng et al. [46] is that we analysed data separately for COVID-19 severity and mortality, while Zheng et al. [46] combined data on COVID-19 critical conditions and mortality. Another previous meta-analysis [44] that included only studies from China reported that comorbid hypertension increased COVID-19 severity by 2-fold, suggesting the prognostic impact of this comorbidity. Our results clearly confirm previous findings and add to them. Li et al. [44] were not able to provide data on cardiovascular comorbidities and death from COVID-19 as data collection was incomplete, and most of the included studies in their analysis did not analyse comorbidities in death cases. Another analysis by Luo et al. [47] included a larger number of studies and found that hypertension was associated with 2.5 times higher odds of mortality; however, considerable heterogeneity was also reported. In this analysis, the relationship between hypertension comorbidity and COVID-19-induced death was pooled using data from China and other countries using a random-effect model to account for heterogeneity. Hypertension was associated with a 3-fold increased fatality rate. The American Heart Association and the American College of Cardiology define hypertension as systolic blood pressure (BP) ≥130 or diastolic BP ≥80 mmHg, and hypertension is a primary risk factor associated with atherosclerotic cardiovascular disease [48]. In line with our analysis, several studies identified high rates of hypertension among severely symptomatic COVID-19 patients [5,12,13]. Roughly half of United States patients with hypertension are prescribed angiotensin-converting enzyme (ACE) inhibitors, aldosterone receptor blockers, and aldosterone antagonists, collectively called renin-angiotensin-aldosterone system (RAAS) inhibitors [49]. The modulator of the RAAS is the ACE2 receptor, which is used by SARS-CoV-2 to bind via its spike (S) protein to allow entry into attached cells. The activation of the RAAS is suggested as a mechanism for severe lung injury, especially in COVID-19 patients [50]. Inhibition of the protective signaling pathways in cardiac myocytes may result in secondary the downregulation of ACE2 expression within the myocardium. Finally, COVID-19 infection induces profound changes in coagulation pathways that create a hypercoagulable state and risk of microvascular thrombosis [51].
A strength of our pooled analysis is that it included more studies than some of the previous ones, and thus a larger sample size from different countries compared to the previous meta-analyses. Hence, our pooled analysis is the most inclusive and up-to-date analysis. The mechanism by which pre-existing cardiovascular disease increases the risk of COVID-19 adverse outcomes is also thought to be through the way that drugs for this disease work [52]. However, studies did not report data on the type of medications prescribed for each comorbidity, and hence we were not able to perform subgroup analyses by medication type. Such analyses are needed in further research. Another strength of this analysis is that visual symmetry in the funnel plot indicates the absence of publication bias. A limitation of this analysis is that most studies did not report the eligibility criteria and whether participants were recruited consecutively. Therefore, selection bias is a likely concern in the included studies. Other biases in the included studies are less likely since all studies sufficiently addressed other points in the JBI tool. Another limitation of this analysis is the possible effect of confounding factors including age, sex, and presence of other comorbidities that contribute to heterogeneity of the included studies. However, we used a random-effect model that addresses heterogeneity.
Conclusion
In summary, the present evidence showed that pre-existing cardiovascular disease in general, as well as hypertension and coronary heart disease, are highly associated with the severity and the mortality rate of COVID-19. Awareness of pre-existing cardiovascular comorbidities is important for the early management of COVID-19.
Supplementary Material
Table S1. Quality assessment of the studies on cardiovascular disease as a comorbidity in coronavirus disease 2019 patients using the Joanna Briggs Institute’s tool. Supplementary data are available at https://doi.org/10.24171/j.phrp.2021.0186.
Quality assessment of the studies on cardiovascular disease as a comorbidity in coronavirus disease 2019 patients using the Joanna Briggs Institute’s tool
Notes
Ethics Approval
Not applicable.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
Authors’ Contributions
Conceptualization: FA; Data curation: FA, SA, MA; Formal analysis: SA; Investigation: FA; Methodology: FA, SA; Project administration: FA; Software: SA; Supervision: FA; Validation: all authors; Visualization: FA, SA; Writing–original draft: FA, SA; Writing–review & editing: all authors.