
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 4(2); 2013 > Article
-
Original Article
Availability of Clean Tap Water and Medical Services Prevents the Incidence of Typhoid Fever - Deog-Yong Leea, Esther Leea, HyeMin Parka, SeongHan Kimb
-
Osong Public Health and Research Perspectives 2013;4(2):68-71.
DOI: https://doi.org/10.1016/j.phrp.2013.03.005
Published online: April 30, 2013
aDivision of Enteric Diseases, Korea National Institute of Health, Osong, Korea.
bDivision of TB and Respiratory Diseases, Korea National Institute of Health, Osong, Korea.
- *Corresponding author. E-mail: leedy0610@korea.kr
• Received: January 8, 2013 • Revised: February 20, 2013 • Accepted: February 27, 2013
Copyright ©2013, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objective:
- In this study, the factors that induced a decrease in the incidence of typhoid fever were analyzed. Based on the study results, we propose a quantitative and concrete solution to reduce the incidence of typhoid fever.
-
Methods:
- We analyzed the incidence and fatality rate of typhoid fever in Korea. Tap water service rate and the number of pharmacies, which affect the incidence rate of typhoid fever, were used as environmental factors.
-
Results:
- To prevent typhoid fever in the community, it is necessary to provide clean tap water service to 35.5% of the population, with an individual requiring 173 L of clean water daily. Appropriate access to clean water (51% service coverage, 307 L) helped the population to maintain individual hygiene and food safety practices, which brought about a decrease in the incidence of typhoid fever, and subsequently a decrease in fatality rate, which was achieved twice. During the 8-year study period, the fatality rate decreased to 1% when the population has access to proper medical service.
-
Conclusion:
- The fatality rate was primarily affected by the availability of medical services as well as by the incidence of typhoid fever. However, an analysis of the study results showed that the incidence of typhoid fever was affected only by the availability of clean water through the tap water system.
- Typhoid is an enteric fever caused by the bacterium Salmonella Typhi and is a common waterborne disease. In 2006, the World Health Organization reported that the estimated incidence of typhoid fever was 10–33 million cases worldwide, with an annual fatality rate of 1.5–3.8% [1]. Typhoid fever outbreaks associated with dirty and contaminated water are continuously reported throughout the world, especially in developing countries [2–4]. Typhoid fever experts have emphasized that appropriate availability of medical services and clean water and individual hygiene practices are required to prevent typhoid fever. However, to date, no one has suggested how much clean water or medical service is needed to decrease the incidence of typhoid fever in a community. Therefore, we analyzed the incidence of typhoid fever, the associated fatality rate, and the factors that induced decreases in the incidence of typhoid fever and deaths in Korea. Based on the results of our analysis, we propose a quantitative and concrete solution to reduce the incidence of typhoid fever.
Introduction
- 2.1. Incidence and fatality rate of typhoid fever
- The incidence and fatality rate of typhoid fever were determined using an online disease statistics system [5] and a communicable disease surveillance yearbook [6], which had a record of communicable diseases from 1961, when such a statistics system was first established in Korea. The incidence rate was calculated by dividing the incidence by the midyear population and multiplying by 100,000 persons. The fatality rate was calculated by dividing the number of deaths by the number of patients and multiplying by 10 to allow graphical comparison with other data.
- 2.2. Environmental factors
- We screened factors to identify those that are related to the decreasing incidence and fatality rate of typhoid fever in Korea. Based on our analysis, public health policy, clean water supply, wastewater treatment, and the availability of medical services, especially antibiotics treatment, were identified as having an impact on the incidence and fatality rate of typhoid. Data on water services, such as tap water service coverage and amounts, were provided by the Korea Water and Wastewater Works Association [7]. However, it was difficult to find data related to public health policy, wastewater treatment, and antibiotic treatment because records of these data were established only after the 1980s, by which the incidence of typhoid fever had already decreased in Korea. As an alternative measure, the number of pharmacies was substituted for the amount of antibiotic treatment, the data of which were provided by the Korea Pharmaceutical Manufacturers [8] and the Korean Pharmaceutical Associations [9]. The saturation was calculated as a relative percentage of a given year: the number of pharmacies in a year divided by the number of pharmacies in 1991.
Materials and Methods
- 3.1. Incidence and fatality rate of typhoid fever
- Approximately 2000–4000 patients were diagnosed with typhoid fever annually since 1961; however, the rate sharply decreased to less than 1000 patients after 1973. After 1977, the incidence of diagnosis was 400 patients, which was similar to the current incidence, reported to be approximately 200 patients annually since 2002, according to an online disease statistics system. The incidence rate decreased to less than 10 persons/100,000 persons after 1971 and remained steady at one person/100,000 after 1977. The number of deaths caused by typhoid fever also decreased gradually; less than 100 people died in 1965, 10 people died in 1973, and only one person died in 1977. There have been no deaths due to typhoid fever in Korea since 1990 except for one case in 2001. The fatality rate decreased in four steps as follows: the first step was a sharp decrease in the rate until 1967, the second step was maintaining the fatality rate at 1% from 1968 to 1975, the third step was a second decrease from 1976 to 1977, and the fourth step was the last turbulent period from 1978 to 1989 (Table 1).
- 3.2. Water service and medical service
- The water service coverage gradually increased from 1961. This was the year when water service statistics were first recorded in Korea. Currently, more than 92% of the population has access to water service; 30 million tons of clean water can be produced and 350 L of tap water can be used per person each day. The number of registered pharmacies has also increased, and currently there are 20,320 pharmacies in Korea. The per capita density of pharmacies was highest in 1991, with 2189 people per pharmacy. The percent saturation of the pharmacy density was calculated based on the per capita density in 1991.
- 3.3. Relationship between typhoid fever and environmental factors
- The decrease in the fatality rate was accompanied by an increase in the percent pharmacy saturation in the early 1960s. The stationary step then began in 1968, and there was a 1% fatality rate for the next 8 years. The second decrease in the fatality rate was accompanied by an end in the decrease of the incidence rate. The decrease in the incidence rate was also accompanied by increases in the percent pharmacy saturation and the water service coverage from 1971 to 1973 (Figure 1). However, the water service coverage might be a more influential factor in the decline of the incidence of typhoid fever, although the correlation coefficients for water service coverage (ρ = −0.84) were similar to that for pharmacy saturation (ρ = −0.85) from 1969 to 1977 (calculated using MS Excel, Microsoft, Redmond, WA, USA).
Results
- The mortality rate of typhoid fever varies between 10% and 32% without treatment but was typically 1–3% if appropriate treatment services were available. The fatality rate gradually decreased after 1961, entered a stationary state in 1968, and remained at 1% for the next 8 years. The increasing availability of medical services, especially improved access to pharmacies, might have induced a greater decrease in the fatality rate than the increasing water service coverage, although it was impossible to correlate the actual use of antibiotics with the fatality rate for typhoid fever. The 1% fatality rate might have been the limit that could be attained with the availability of medical services during the 8-year period. During this period, 7674 pharmacies serviced the community, and each pharmacy provided medicines to an average of 4019 people. These data may vary with the population and geography in each country. However, these data suggest that there is a critical point in the availability of medical services that must be reached to decrease the fatality rate of typhoid fever.
- The second decrease in fatality rate began in 1976, when the incidence rate decreased to less than two persons/100,000 persons. The incidence rate decreased to less than 10 persons/100,000 persons after 1971, but was not this low in 1968, when the 1% fatality rate was reached. The availability of medical services might be the primary factor responsible for the first decrease in the fatality rate. The incidence rate decreased to less than 10 persons/100,000 persons after 1971. However, the fatality rate dropped to 1 percent in 1968. However, the absolute decrease in the incidence rate might act as a secondary factor that led to the decreased fatality rate.
- Tap water service provided clean water to 35.5% (1971), 38% (1973), and 51% (1977) of the population, and one person was able to access 173 L (1971), 179 L (1973), and 304 L (1977) of clean water daily. At these time points, the incidence and incidence rate changed abruptly; the incidence rate fell below 10 persons/100,000 persons in 1971, below 1000 persons in 1973, and below one person/100,000 persons in 1977. These data suggest that to prevent typhoid fever in the community, it is necessary to provide clean tap water to 35.5% of the population and at least 173 L of clean water per person every day. An appropriate availability of clean water (51% service coverage, 307 L) allowed the population to maintain individual hygiene and food safety practices, which resulted in a decrease in the incidence of typhoid fever and the second decrease in the fatality rate. In 1971, the fatality rate was already maintained at the 1% rate by providing proper medical services, but the water service coverage continuously increased. Therefore, an adequate amount of clean water was the primary and most important factor in preventing typhoid fever.
- This study could not determine the effects of public health policy, wastewater treatment, and accurate antibiotic treatment to treat patients with typhoid. However, these limitations did not greatly hinder our analysis because an increase in wastewater treatment was generally accompanied by an increase in the supply of tap water, and the number of pharmacies could be used as a representative marker of antibiotic treatment before the separation of dispensary from medical practice. Public health policy included patient separation, carrier and food handler management, and a vaccine program, but it was not easy to evaluate the quantitative effect of these policies on the incidence of typhoid fever. However, the next generation should work to eradicate typhoid fever because imported cases and carrier management are still persisting problems in developed countries.
Discussion
-
Acknowledgements
- We thank the Korea Water and Wastewater Works, the Korea Pharmaceutical Manufacturers, and the Korean Pharmaceutical Associations for providing data. This study was supported by grants from the Elimination Program of Endemic Diseases in Korea.
- 1. Farooqui A, Khan A, Kazmi SU. Investigation of a community outbreak of typhoid fever associated with drinking water. BMC Public Health 2009;12;9:476PMID: 20021691.ArticlePubMedPMC
- 2. Ghenghesh KS, Franka E, Tawil K, et al. Enteric fever in Mediterranean north Africa. J Infect Dev Ctries 2009;12;3(10). 753−61. PMID: 20009276.ArticlePubMed
- 3. Karkey A, Aryjal A, Basnyat B, et al. Kathmandu, Nepal: still an enteric fever capital of the world. J Infect Dev Ctries 2008;12;2(6). 461−5. PMID: 19745524.PubMed
- 4. Beyene G, Asrat D, Mengistu Y, et al. Typhoid fever in Ethiopia. J Infect Dev Ctries 2008;12;2(6). 448−53. PMID: 19745522.ArticlePubMed
- 5. KCDC. Typhoid fever [Internet] [cited 2010 July]. Available from: http://stat.cdc.go.kr (Accessed 20.07.2010).
- 6. KCDC. Communicable disease yearbook. Seoul: KCDC; 2007.
- 7. KWWA. Annual report of tap water supply. Seoul: Korea Water and Waterwaste Works Association; 2010.
- 8. KPMA. The 50th history of pharmaceutics in Korea. Seoul: Korea Pharmaceutical Manufacturers Association; 2010.
- 9. KPANET. The 50th history of pharmaceutics in Korea. Seoul: The Korean Pharmaceutical Association; 2010.
References
Figure 1Relationships of the incidence and fatality rate of typhoid fever with factors inducing decreases in these values in Korea. The fatality rate decreased in two steps. The first step was the result of the increased availability of medical services, and the second was the result of the decreased incidence rate. The incidence rate abruptly decreased from 1971 to 1973; this decrease was only affected by the water service coverage. Closed squares and line = incidence rate; closed circles and line = fatality rate multiplied by 10; open squares and line = water service coverage; open circles and line: pharmacy density divided by greatest pharmacy density over time to yield a percentage.
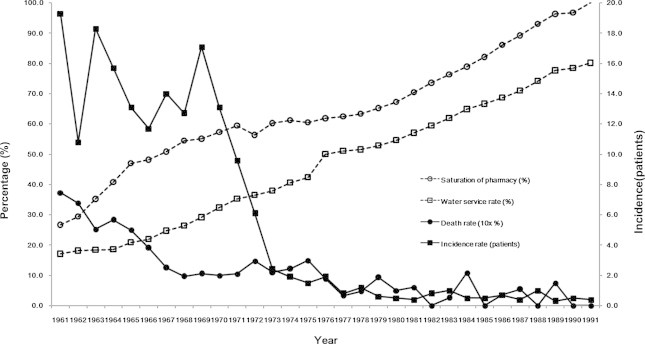
Table 1Effect factors and affect zone for the prevention of typhoid fever in the community
Figure & Data
References
Citations
Citations to this article as recorded by 
- TIPICO X: report of the 10th interactive infectious disease workshop on infectious diseases and vaccines
Irene Rivero-Calle, Jose Gómez-Rial, Louis Bont, Bradford D. Gessner, Melvin Kohn, Ron Dagan, Daniel C. Payne, Laia Bruni, Andrew J. Pollard, Adolfo García-Sastre, Denise L. Faustman, Albert Osterhaus, Robb Butler, Francisco Giménez Sánchez, Francisco Álv
Human Vaccines & Immunotherapeutics.2021; 17(3): 759. CrossRef - Progress in the overall understanding of typhoid fever: implications for vaccine development
Peter J O’Reilly, Dikshya Pant, Mila Shakya, Buddha Basnyat, Andrew J Pollard
Expert Review of Vaccines.2020; 19(4): 367. CrossRef
 PubReader
PubReader Cite
Cite
