Health-Related Quality of Life Based on Comorbidities Among Patients with End-Stage Renal Disease
Article information
Abstract
Objectives
The aim of this study was to investigate comorbidities in patients with end-stage renal disease, and to compare health-related quality of life (HRQOL) according to the type, and number of comorbidities.
Methods
A total of 250 adults undergoing hemodialysis were recruited at local clinics. HRQOL was measured using the 12-item Medical Outcomes Study Short Form questionnaire. Data were analyzed using descriptive statistics, analysis of variance, and t test.
Results
Around 70.8% of patients with end stage renal disease had 1 or more comorbidities, and the most common comorbidities were hypertension, diabetes, and cardiovascular disease. HRQOL was significantly different based on the number of comorbidities (F = 9.83, p < 0.001). The effect of comorbidities on the scores for mental health domains of the HRQOL questionnaire was not conclusive compared with the scores for the physical domain which were conclusive. Among the comorbidities, diabetes was associated with a lower quality of life.
Conclusion
The customized management of diabetic and hypertensive patients is necessary for the early detection and prevention of chronic kidney disease, and slowing the progression of renal disease and managing cardiovascular risk factors is essential.
Introduction
Chronic kidney disease (CKD) is a serious disease, with a high prevalence and high socio-economic burden worldwide. However, in the absence of distinct symptoms, patients with CKD are typically miss the optimal treatment period due to late detection [1]. In end stage renal disease (ESRD), there is a reduction in kidney function requiring the patient to receive renal replacement therapies, such as hemodialysis, peritoneal dialysis, or kidney transplantation. The number of patients with ESRD in Korea was 2,500 in 1986 however, this has increased by 10% annually since 2001, and in 2018, there were 17,621 new cases of ESRD [2]. The increase in incidence of ESRD in Korea is faster than in other countries thus, early detection of CKD and prevention of the associated complications are urgently required [1,3].
Comorbidity is the presence of a co-existing or additional condition or disease in addition to the specific disease of interest [4]. Comorbidities can be used as a diagnostic indicator because they can affect the patient’s capacity to function and survive [5]. Patients with comorbidities have complex interactions between a co-existing disease and a disease of interest, leading to late diagnosis and difficulties in treatment which may cause a high degree of disease severity [5,6]. Under these circumstances, the patients’ use of health care services would increase, and health outcomes such as mortality may be affected [7]. At the same time, comorbidities can affect a patient’s life leading to limitations in physical function, disabilities, psychological problems, and an increasing economic burden [8,9]. In other words, comorbidities affect the physical, psychological, and social aspects of life, thus reducing quality of life (QOL) [9,10]. The health-related quality of life (HRQOL) questionnaire is an important indicator for the effect of disease on a patient’s life [11,12]. Various factors related to HRQOL of patients with ESRD have been reported [13]. However, the health outcomes due to comorbidities are not well-understood, and the systematic management of comorbidities is insufficient.
The most common accompanying conditions and diseases among patients undergoing dialysis are hypertension, diabetes, coronary artery disease, congestive heart failure, hepatitis B, and cerebrovascular disease [2]. Patients who develop ESRD are more likely to have diabetes or hypertension. Among the major causes of ESRD, diabetic nephropathy accounts for 48.8%, and hypertensive nephropathy accounts for 19.8% of newly diagnosed patients in Korea in 2018 [2]. These data indicate the importance of diabetes and hypertension management in ESRD. Around 33.7% of patients receiving dialysis for ESRD died of complications due to cardiovascular disease in 2018 [2]. Therefore, the effect of cardiovascular disease on the clinical prognosis of patients with ESRD must be considered [14].
Multimorbidity occurs when an individual is affected by 2 or more chronic diseases [10]. A considerable number of patients with ESRD have multimorbid conditions [1–3,14]. The prevalence of multimorbidity is increasing because of population aging, and the burden of diseases is increasing due to multimorbidity worldwide [5]. In this context, the Organization for Economic Cooperation and Development has indicated that multimorbidity is 1 of the most important new challenges that should be addressed by its member countries [6]. In Korea, disease burden is expected to be extremely high due to complex chronic diseases [9]. Considering that the primary care system is not well-established, the effects of multimorbidity on the health outcomes of patients will be severe. Until now, the interactions or cumulative effects of various diseases have not been considered because patients have been treated through a single disease-focused method [10]. In addition, patients are not provided with adequate information on how to manage multimorbidity, and which diseases should be prioritized [4,9,15]. The number of patients with multimorbidity is expected to increase due to various complications resulting from ESRD or disease progression due to underlying conditions or diseases such as diabetes or hypertension.
This study aimed to identify the distribution of comorbidities of patients with ESRD and to determine whether there is a correlation between the number of major comorbidities and HRQOL. The results of this study may contribute to the management of multimorbidity in patients with ESRD.
Materials and Methods
1. Participants
Participants were adults aged 18–65 years who were undergoing hemodialysis regularly (2–3 times a week, for 6 months or more) at a local dialysis clinic. The number of participants required for this study to be meaningful was 207, which was calculated using the G-power 3.1 program, with a median effect size of 0.25, a significance level of 0.05, and power of 0.90 for all 3 groups (0, 1, and 2 or more comorbidities). A total of 250 participants were included in the study.
2. Measurements
2.1. Comorbidity
Comorbidity indicates that there are 1 or more additional diseases that co-occur with a primary disease [10]. In this study, diabetes, hypertension, cardiovascular disease (congestive heart failure, arrhythmia, coronary artery disease), and other diseases including hepatitis B and C, cancer, gout, and gastrointestinal diseases which were observed in patients with ESRD, were investigated.
2.2. HRQOL
The HRQOL questionnaire is an assessment of overall health where each individual’s response to the physical, mental, and social consequences of illness in daily life is measured [11]. In addition, the 12-item Medical Outcomes Study Short Form (SF-12) questionnaire was used in this study [12]. The SF-12 instrument was designed for use in clinical practice, research, and health policy evaluations with the aim of reducing a respondent burden, while achieving minimum standards of precision, for the purposes of group comparisons involving multiple health dimensions. Permission to use the tool through Quality Metric Incorporated was received. This tool consisted of 12 items in 8 sub-domains. There were 2 main components consisting of a physical health summary (physical function, physical role limitation, pain, and general health) and a mental health summary (vitality, social functioning, emotional role restriction, and mental health). The scores for each item ranged from 3 to 5 with a higher score indicating a better HRQOL.
3. Statistical analysis
This study was a secondary analysis following the previous study [16]. Primary data were collected from a study about the self-management and QOL of hemodialysis patients between 2013 and 2014 using a self-reported questionnaire. Patients agreed to participate in the study, and written consent was obtained by the investigator before the survey began. A waiver approval (no.: 2017–0013) from the K University Institutional Review Board was received. The collected data were analyzed using SPSS software (version 23.0; IBM Corp., Armonk, NY, USA). Participants’ characteristics were analyzed using descriptive statistics. The reliability of the measurement was calculated using Cronbach’s α which was measured as 0.85. One-way analysis of variance was used to compare HRQOL among the 3 groups according to the number of comorbidities other than ESRD (0, 1, and ≥ 2 comorbidities). For significant variables, Scheffe’s post-test was used to determine the magnitude of difference. In addition, HRQOL with or without diabetes, hypertension, and cardiovascular disease was evaluated by the Independent t test. Statistical significance was achieved with p < 0.05.
Results
1. Demographic characteristics
The mean age of the 250 patients was 47.6 ± 9.3 years, and 40–49 years age group accounted for the most participants (n = 96). Among the participants, 71.2% were males, and 54.8% were married. A total of 138 (55.2%) patients had secondary school education (≤ 12 years). In addition, 119 (47.6%) patients had a monthly family income ≤ 2 million Korean won, and 126 (50.4%) patients had a job (Table 1).

Demographic characteristics (N = 250).
2. Disease-related characteristics and comorbidities
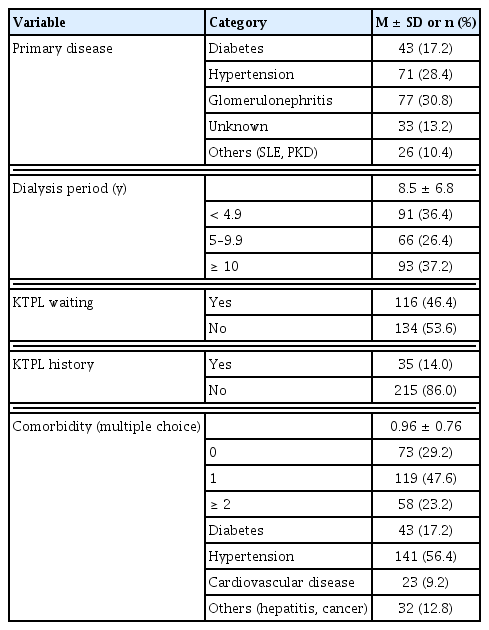
The most common cause of chronic renal failure was glomerular disease (30.8%) followed by hypertension (28.4%), and diabetes (17.2%). The mean duration of dialysis was 8.5 ± 6.8 years, with 93 (37.2%) patients being on dialysis ≥ 10 years. A total of 116 (46.4%) patients were waiting for kidney transplantation, and 35 (14.0%) patients had received a kidney transplant in the past.
The most common comorbidities were hypertension (56.4%), diabetes (17.2%), and cardiovascular disease (9.2%). The mean number of comorbidities was 0.96 ± 0.76, with 73 (29.2%) patients having no comorbidities. Other diseases were hepatitis (B and C types), cancer, gout, and gastrointestinal diseases (Table 2).
Disease-related characteristics and comorbidities (N = 250).
3. HRQOL of patients with ESRD based on the number of comorbidities
The participants were divided into 3 groups according to the number of comorbidities they were living with. In the 3 groups, there were 73 patients with ESRD and no comorbidities, 119 patients with 1 comorbidity, and 58 patients with ≥ 2 comorbidities. A comparison of HRQOL of the 3 groups (based on the number of comorbidities) showed that there was a significant difference among the 3 groups in both the scores for the physical and mental health domains of the questionnaire, and overall HRQOL. The scores for the physical health domains (F = 12.83, p < 0.001) showed a larger difference compared with the scores for the mental health domains (F = 5.37, p = 0.005). There was a significant difference in HRQOL according to the number of comorbidities (F = 9.83, p < 0.001; Table 3).
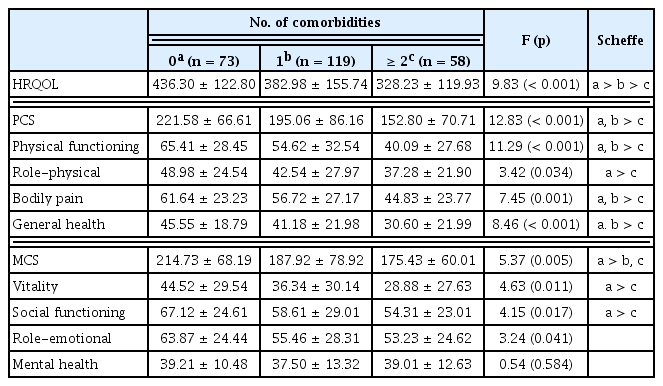
Comparison of health-related quality of life in 3 groups.
4. HRQOL of patients with ESRD based on the comorbidity type
Among patients with ESRD, HRQOL was compared based on the presence of diabetes, hypertension, and cardiovascular disease. In comparison with patients without diabetes, those with diabetes had significantly lower scores for overall HRQOL (t = 2.69, p = 0.008) and physical HRQOL (t = 3.27, p = 0.001). The scores for overall HRQOL (t = 2.25, p = 0.025) and physical HRQOL (t = 2.49. p = 0.014) were also significantly lower among patients with hypertension compared with those without hypertension. In comparison with patients without cardiovascular disease, patients with cardiovascular disease had significantly lower scores for physical HRQOL (t = 2.25, p = 0.025; Table 4).

Comparison of health-related quality of life based on major comorbidities.
Discussion
In this study, the impact of comorbidities on HRQOL of patients with ESRD were investigated to address the issue of increasing multimorbidity. The average number of comorbidities suffered by patients in this study (alongside ESRD) was 0.96, ranging from 0 to 3 comorbidities. The most common comorbidity was hypertension. For the single disease group, 73 (29.2%) patients with ESRD were included. Diabetes did not occur in the progressive stage of kidney disease, with the exception of 17.2% of patients who had diabetes as a primary disease. Hypertension is 1 of the major causes of kidney disease and may result from decreased kidney function. Therefore, control of blood pressure is important for the prevention and management of kidney disease. Shim [17] reported that the mean number of comorbidities in elderly hemodialysis patients (with an average age of 71.2 years) was 2.93 (the highest number of comorbidities was 10). Around 14.2% of patients had ESRD without comorbidities. In addition, there were more than 4 diseases in 32.1% of cases, which were the most common cases. Considering that the mean age of patients in this study was 47.6 years, disease management should be initiated as early as possible to prevent the occurrence of age-related co-existing diseases that may develop.
The incidence of cardiovascular disease in patients with ESRD in this study was lower (9.2%) than a previously reported study where Korean patients who underwent hemodialysis accounted for 18.8% of patients who had cardiovascular disease [2]. This result may be attributed to convenient sampling, which involved the voluntary participation of patients who were in a relatively stable state of health. The heart and kidneys are pathophysiologically related organs and if dysfunction occurs in 1 the other organ is also simultaneously affected. Patients with CKD have been reported to have a cardiovascular mortality rate 10 to 20 times higher than the rate in the control group of the same age and gender [18]. The risk of cardiovascular disease is also increased in patients with early onset CKD. Therefore, a multidisciplinary approach is needed for the appropriate management of CKD.
This current study compared HRQOL based on the number of comorbidities in each group. A large difference was observed in the scores for the physical health domains between groups. However, there were relatively few differences in the scores for the mental health domains. Fortin et al [19] examined the relationship between multimorbidity and QOL in the primary care settings. An inverse correlation was reported between the number of diseases and the scores for the physical domain of the QOL questionnaire. For the QOL scores in the social and psychological domains, the relationship was less clear, which was consistent with the findings of this current study. In addition, Manns et al [13] examined the comorbidities and QOL of patients undergoing dialysis. The SF-36 scores, which are a measure of HRQOL, were significantly lower as the number of comorbidities increased. Kim and Kim [20] reported that comorbidity was the most influential variable in the analysis of factors affecting the QOL of hemodialysis patients in Korea.
From the perspective of chronic inflammation and health, the levels of inflammatory proteins such as interleukin-6, and C-reactive protein were relatively high in chronic diseases such as cardiovascular disease, hypertension, and diabetes [21] and predicted adverse health outcomes, such as mortality. Additionally, the higher the level of proinflammatory cytokine IL-6, the more severe the symptoms of depression [22]. The relationship between inflammation and negative health outcome was strong for cardiovascular events or all-cause mortality in the elderly [23]. The results observed in this current study showed the greater the number of comorbidities a patient has, the lower the score achieved in the HRQOL questionnaire. Therefore, active disease management strategies are needed to prevent comorbidity.
Diabetes was adversely associated with HRQOL of patients with ESRD in this study. Diabetic nephropathy is a major complication in 20–40% of diabetic patients causing ESRD [24]. Diabetes is a chronic disease that requires constant management [25], and for patients who are socially active, they may experience psychological constraints and conflicts due to dietary restrictions, repeated blood glucose testing, medication requirements, and insulin injections. In addition, ESRD with diabetes has a greater economic burden arising from medication, and hospitalization which is 1.6 times higher in patients compared with ESRD patients without diabetes [24]. Therefore, strategies to either prevent the onset of diabetes in ESRD, or initiate early treatment in diabetic patients to prevent progression to ESRD are crucial.
The scores for physical HRQOL of patients with ESRD who had hypertension or cardiovascular disease, were significantly lower in this study. Hypertensive patients may attempt to regulate blood pressure to prevent complications such as a stroke, when performing tasks in daily life or the workplace [26]. Patients with cardiovascular disease, such as coronary artery disease, heart failure, and arrhythmia, are limited in physical activity due to lower cardiac function, resulting in a lower QOL [27,28]. Cardiovascular factors, such as arrhythmia and myocardial infarction, are the major causes of death among hemodialysis patients [14] thus, active management of these conditions is essential. Patients with ESRD should be encouraged to self-manage the risk factors, such as diet, blood pressure, and water intake, which are associated with developing cardiovascular disease.
Although comorbidities have a negative effect on health, the progression of kidney damage due to diabetes and hypertension can be delayed through early detection and appropriate treatment, and self-management approaches [29]. However, only 20% of patients with moderate renal dysfunction are aware of self-management approaches to their disease, and patients are typically not satisfied with the early diagnosis and treatment of CKD complications [1,3]. Chin et al [3] reported that awareness of kidney disease among patients with CKD was only 6.3%. Although CKD causes various health problems, a low awareness of the disease can interfere with the control of blood pressure and blood glucose, which are important for inhibiting the progression of CKD. In diabetic patients, renal function evaluation is recommended every year however, this evaluation of kidney function is not performed for many diabetic patients in Korea [24]. Therefore, more education on CKD should be delivered for the benefit of the public and medical staff. In addition, awareness of the importance of the early diagnosis of kidney disease and management of kidney disease complication should be improved.
In conclusion, around 70.8% of patients with ESRD had ≥ 1 comorbidities, and the scores for HRQOL were significantly different based on the number of comorbidities. Among the major comorbid diseases, diabetes had the greatest effect upon ESRD. In the future, patients with more than 2 chronic diseases should be systematically evaluated. In addition, it is necessary to consider the social and psychological effects on the patient’s health, while developing a system to identify and share the treatment plan with various medical staff. In this study, the self-report method was used to measure comorbidities. However, to obtain comprehensive and systematic results that reflect the severity of the disease, tools such as the Charlson comorbidity index [30] and index of co-existent disease [31], are recommended in future studies. We performed a convenience sampling of adult dialysis patients residing in local areas. Therefore, caution should be exercised when generalizing the results of this study. The effects of multimorbidity on the health outcomes in the patients with ESRD were shown in this study using a different approach from the conventional single disease-centered approach.
Acknowledgments
The authors would like to thank the patients for participation in the present study.
The study has been approved by Kyungpook National University Institutional Review Board (no.: 2017-0013).
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.