The Moderating Role of Social Activity on Age Norms and Subjective Health Status of Older Adults: A Two-Stage Cluster Korea National Survey
Article information
Abstract
Objectives
This study aimed to examine how social activity (SA) moderates the relationship between age norms (AN) and subjective health status (SHS) among older adults in Korea. Based on the theories of age-integrated structure and active aging, the proposed hypotheses were that SHS has a positive association with attitudes towards AN, and with the interactions between different types of AN and SA.
Methods
Cross-sectional data from a Korean national survey of older adults were analyzed. Participants were older adults N = 10,451, of whom 10,280 were used in the study sample. Multivariate linear regression including interaction terms, was used to examine the associations among SHS, AN, and SA.
Results
The results of multivariate linear regression examining learning (ß = 0.066, p < 0.001), working (ß = 0.063, p < 0.001), and remarriage (ß = 0.036, p < 0.001) showed that those who perceived AN more positively, were more likely to have a high SHS. With interaction terms, those who had a positive attitude towards AN for learning and volunteering (ß = 0.025, p < 0.05), and remarriage and engaged in friendship groups (ß = 0.032, p < 0.05) were more likely to have a high SHS.
Conclusion
SA serves as a great moderator between AN and SHS.
Introduction
Aging is one of the leading issues of social transformation globally and can be observed in the rapidly expanding, aging population of South Korea. According to the U.S. Census Bureau 2015, South Korea is predicted to have the second highest percentage (35.9%) of elderly people in the population by 2050 following Japan (along with Hong Kong, Taiwan, and Thailand) [1]. Radical transformation in Korea brought about by economic and technological growth, has brought changes in social structures with new cultural values being adopted, and some traditional values being disregarded [2]. Korea is generally known as one of the Asian countries where respect for the elderly is practiced as a social norm. However, this paradigm is shifting as Korean people adopt Western culture, and attitudes towards the aging and the elderly have changed [3–5]. The majority of the older generation (≥ 65 years) believe in Confucian and communism which typically create conflict with the younger generation over sociocultural issues, values, perceptions, and attitudes [2]. Since the 19th century, there have been thoughtful discourse over generational differences, but no clear classification of these differences or proposed resolutions have been made [6].
According to Atchley [7], individuals’ thoughts and behavior towards aging were influenced by age norms (AN) which are defined as social rules for age-appropriate behavior, socially expected roles, and the timing of life events [8,9]. AN set out the demeanor of the social roles of individuals in a given life stage, and operate with assumptions and expectations based on culture and tradition [7]. Elderly Koreans today may face more social restraints resulting in negative AN, although the notion of respect for elders is still practiced in Korea like in other Eastern societies [10,11]. Indeed, social expectations for the elderly may act as a structural barrier or social coercion, when they conflict with the preferences and desires of the elderly [5]. As a result, the quality of life for the elderly population may be reduced. It is noteworthy that a negative AN (ageism) was observed to be a negative factor that influenced mental health and quality of life among the elderly Korean population [12,13]. The aging process concerned with social structure, has a significant influence on the psychological condition and physical activity of older adults [14,15]. Hence, a positive AN could be beneficial for subjective health status (SHS), whereas a negative AN could be associated with a poor health status in later life. SHS refers to how individuals evaluate their general or physical health [14]. However, there are few studies regarding the impact of positive and negative AN that are ingrained in the minds of elderly Koreans, which can contribute to the health elderly people [4]. In Western society, social engagement was observed to be associated with a better physical and mental health among older people [14,16,17]. Similarly, social participation programs were found to bring empowerment and increase the life satisfaction of elderly Koreans with poor health [15,18]. However, in the rapidly expanding, aging population of South Korea there are limited studies regarding participation of the elderly in social activities (SA) who may have been exposed to positive or negative AN.
In this study, the focus was on examining the relationship between older adults’ attitudes towards AN and their SHS based on the concept of age-integrated structures (emphasizing heterogeneity in healthy aging over the areas of education, work, and leisure without age discrimination) and active aging (being given opportunities throughout life and maintaining formal or informal activities in later life) [19,20]. Additionally, identification of the moderating role of a SA between these relationships was addressed. Although these questions on relatively similar phenomena, have already been reported for Western societies, the aging process concerning the social structure, and the subjective health of older adults in modern Korean society, have not yet been investigated in detail. As “rapid aging” is a shared concern among Asian countries (who will globally rank high in the number of elderly in the population by 2050 [1]), it is necessary to address this burden.
Based on the theories and concepts of AN, age-integrated structures, active aging, hypotheses and a research model were developed with the assumptions that positive and open attitudes towards AN are associated with a better SHS among older adults in Korea (Figure 1). Additionally, the outcomes were expected to be influenced by the interaction between AN and SA. These assumptions were tested across representative data from a Korean national survey (2014) of older adult (≥ 65 years) participants (N = 10,451). The questionnaire included the areas concerned with learning, working, remarriage, and different types of social participation [21].
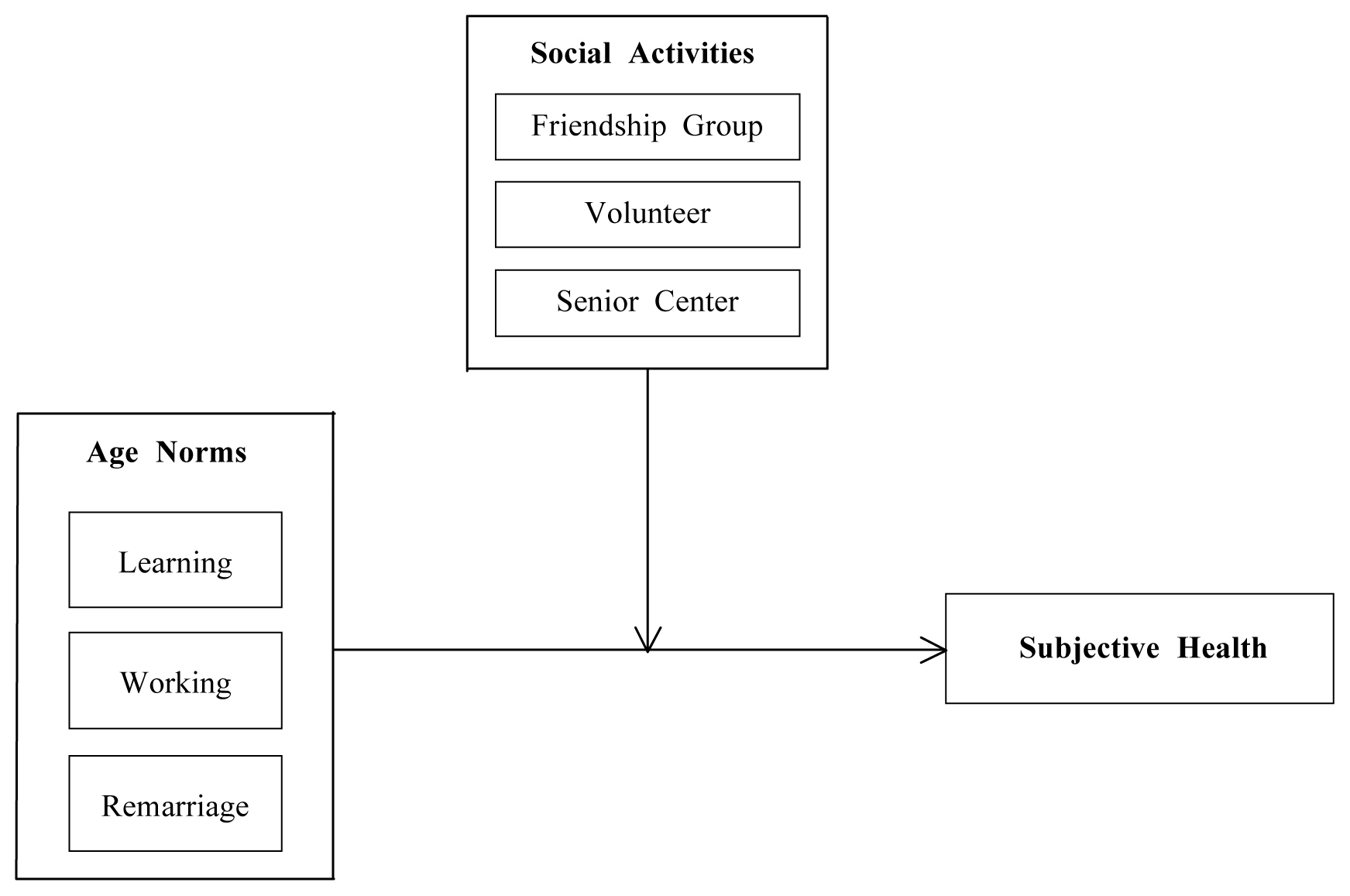
Research model.
Materials and Methods
1. Sampling and data collection
This cross-sectional study used data drawn from a 2014 Korean national survey of older adults, established by the Ministry of Health and Welfare [21]. The data collection period was between March 2014 and December 2014. The target population for the primary survey was the elderly aged ≥ 65 years who resided in a general residential facility, there were 16 cities and provinces surveyed, excluding those who live in dormitories, specialized facilities, and island areas. The sampling scheme was a stratified 2-stage cluster extraction. The primary sampling unit was 90% of the population and housing survey 2010. The secondary sampling unit was all the older adults aged ≥ 65 years living in the survey area. The data were collected through face-to-face interviews by the interviewers who were trained by the research team of the study. Participants were older adults N = 10,451, of whom 10,280 were used for analyses in this study. Some cases (n = 171) with missing values or lack of responses for the study variables were excluded.
2. Measures
The outcome variable was SHS, and it was measured by the question, “What do you think about your health condition compared to your peers?” The response scale ranged from 1 = very good to 5 = very bad, (including physical and emotional health compared with their peers). In this study, a reverse-coded score was used for convenience of interpretations; the higher the SHS score, the better the health.
The independent variable was the attitude towards AN, and was measured over 3 subscales: learning, working, and remarriage. The questions asked were; 1) Do you agree with the elderly learning something new? 2) Do you agree with the elderly working? and 3) Do you agree with the elderly remarrying?” for AN towards learning, working, and remarriage respectively. The response scale ranged from 1 = strongly agree to 5 = strongly disagree. In this study, a reverse-coded score was used for convenience of interpretations; the higher the score, the more positive the attitude towards AN.
Regarding the moderator, engagement in a SA was measured over 3 subscales, friendship group, volunteer activity, and senior center participation. For the friendship group, a dichotomous scale was used for the question, “Have you been involved in friendship group in the past year?” For the volunteer activity, a dichotomous scale was used for the question, “Have you ever carried out volunteer work in the past year?” For senior center participation, a dichotomous scale was used for the question, “Have you participated in a senior community center in the past year?” Other factors found to influence the outcomes, including gender, age, education, family status, and limitations in activities of daily living, were adjusted for the analyses. Additionally, the variables, attitudes towards AN and SA, were mean centered on reducing multi-collinearity when the variables were used as interaction terms for moderate effect.
3. Ethics statement
The Ministry of Health and Welfare sent a letter explaining the purpose of the national legal survey to the resident autonomy center of the survey area. Also, informed consent was obtained from all participants before the interview. In addition, the study was approved by the institutional review board of K University (IRB No.: 17-EX-41-A-1).
4. Statistical analysis
Descriptive statistics and frequencies were run for all variables. Pearson’s correlation coefficient was employed to establish whether the continuous variables of the study were correlated and multivariate linear regression models for SHS with increasing significance values, after controlling for potential confounders, was performed. Values of p < 0.05 were considered to be statistically significant. Associations amongst attitudes towards AN, SA, and SHS were examined, followed by modeling including interaction terms for attitudes towards AN and SA. Statistical analyses were conducted using SPSS version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Table 1 represents general characteristics of the study sample n = 10,280 participants. There were 59.0% who were females, and the study sample ages were 70–74 years (32.0%), 75–79 years (26.6%), and 6–69 years (21.9%). The mean age of the study participants was 73.89 years with a range between 65–105 years. The study sample education level was elementary school education (30.6%) followed by those with no education (26.3%), high school graduates (18.9%), middle school graduates (14.6%), and those with college degrees or higher (9.7%). The family status of the participants who had partners was 52.7% followed by those who lived alone (27.3%), those who lived with children (16.1%), and others [i.e., relatives or friends (4.0%)]. Most respondents (95.0%) were completely independent in their activities of daily living. Regarding attitudes towards AN for learning, working, and remarriage, the average scores (± SD) were 3.67 ± 0.81, 3.61 ± 0.86, and 2.42 ± 0.93, respectively. Regarding participation in a SA, the percentages of participants who engaged in a friendship group, experienced volunteering, or participated in a senior community center were 42.6%, 17.8%, and 37.7% respectively. Regarding SHS, respondents perceived their health as good (33.9%) or bad (33.5%), and the average score was 2.92 ± 1.02.
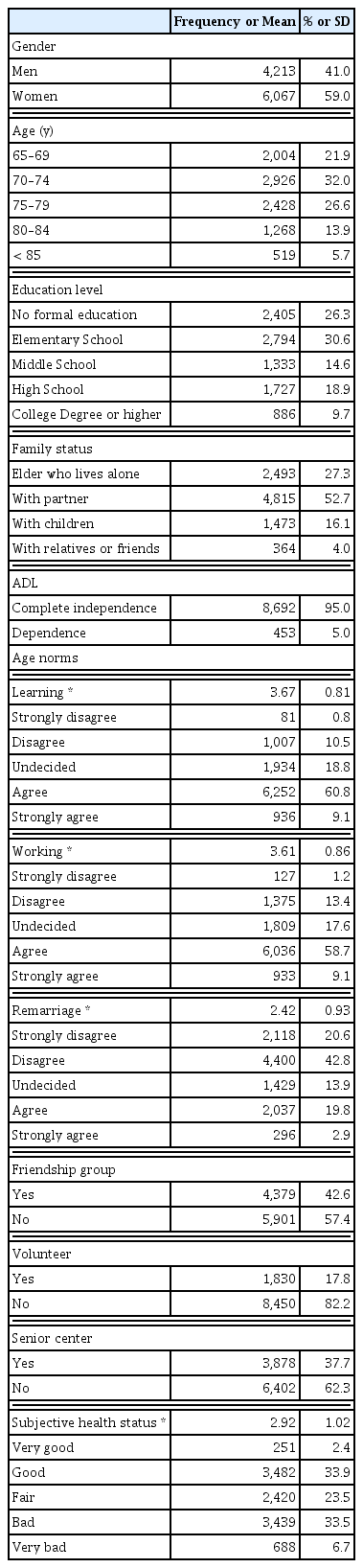
Sample characteristics and variables in the model (n = 10,280).
The 3 subscales regarding attitude towards AN showed a significantly weak positive correlation (Pearson’s correlation coefficients 0.296–0.397). It was confirmed that there was no multicollinearity between variables. Additionally, there was a significantly weak positive correlation between SHS and learning (r = 0.155), working (r = 0.133), and remarriage (r = 0.119).
Gender, age, education level, family status, and limitations in activities of daily living were controlled for in the analysis (Table 2). The level of activities of daily living was assessed using 7 self-care activities (e.g., dressing, face washing and shampooing, bathing, eating, mobility, using the toilet, controlling bladder and bowel functions) and it was rated as either fully independent, partial-help, or dependent. Those who perceived AN more positively for learning (ß = 0.066, p < 0.001), working (ß = 0.063, p < 0.001), and remarriage (ß = 0.036, p < 0.001) were more likely to have a high SHS, as shown in Model 1. The coefficient of determination of the model was increased by 1.2 % when the experience of a SA was added into Model 2. The analysis revealed that those who engaged in friendship group (ß = 0.111, p < 0.001), and who participated in volunteering (ß = 0.028, p < 0.01) were more likely to have a high SHS, as revealed in Model 2. The association of the model with interaction terms was retested as shown in Model 3: Those who had positive attitudes towards learning, and who engaged in volunteering were more likely to have a high SHS (ß = 0.025, p < 0.05). In the same way, those who had more positive attitudes towards remarriage, and who engaged in a friendship group were more likely to have a high SHS (ß = 0.032, p < 0.05). On the other hand, those who had negative attitudes towards learning and who engaged in volunteering, reported their health condition as worse than those who had negative attitudes towards learning and did not participate in volunteer activities. Whereas, the same trend was not found in the interaction between remarriage and friendship group, as shown in Figure 2.
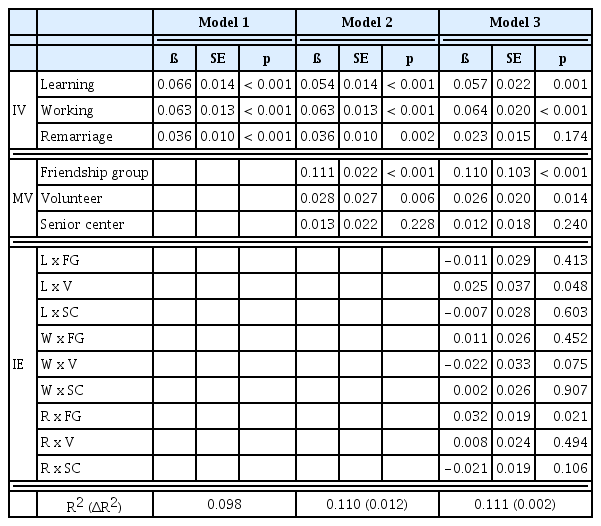
Regression models on age norms, social activities, and subjective health status.
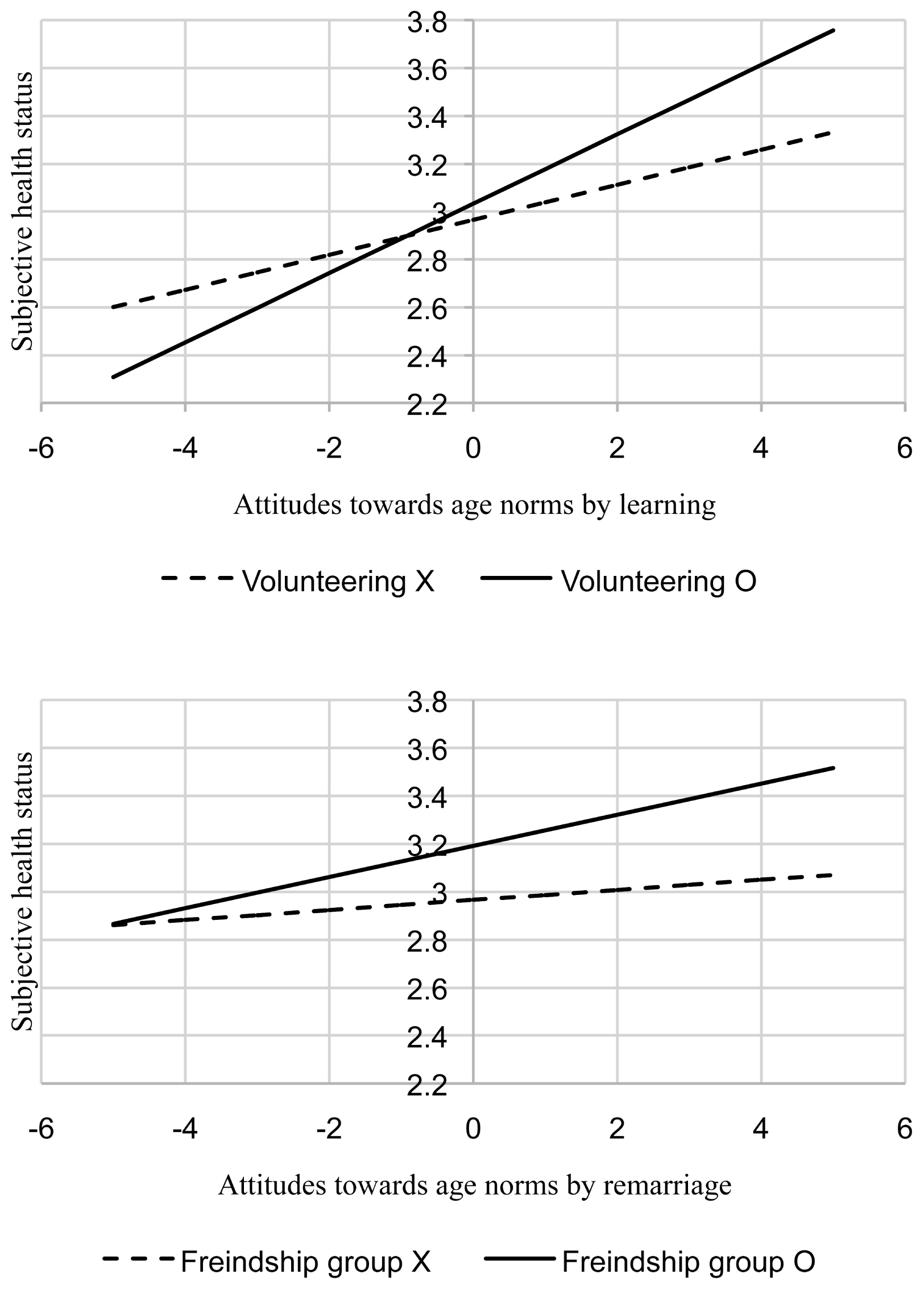
Interaction effect.
Discussion
This study examined the relationship between attitudes towards AN and SHS, and the moderating role of a SA between these relationships using Korean national data for adults ≥ 65 years. It was assumed that positive attitudes towards AN would be associated with a better SHS. Additionally, it was anticipated that these relationships would be influenced by the interaction effects between AN and SA. The study revealed that 2 sub-variables of AN, learning and working, were significantly associated with high levels of SHS in older Korean adults. This indicated that learning in old age is vital at increasing the quality of life and confidence in health management, and these observations were consistent with the findings reported in the Western world [22–24]. In the same way, working or having multiple roles in old age, was shown to play an essential role for healthy aging and independence [25,26]. Although the causality between healthier older adults and their active social involvement is acknowledged, the focus of the present study was more involved with the interplay between different kinds of AN, and social participation that was measured as important to elderly Koreans ≥ 65 years in 2014.
In addition, the associations between AN and SHS were moderated through SA, partly in line with the study assumptions. In detail, 2 moderating sub-variables, friendship group and volunteering, presented greater positive interaction effects with learning and remarriage, where higher levels of SHS were reported. In other words, SHS was more likely to be enhanced when an older adult perceived learning positively and took part in volunteering. Equally, SHS would become greater if an older adult regarded remarriage in old age positively and engaged in a friendship group. The observations in this study supported age heterogeneity where the theories of age-integrated structures and active aging, are reliable predictors of successful and healthy aging [19,20,27]. It is important to note that positive attitudes towards remarriage did not show a direct association with the SHS of older Korean adults unlike some Western studies where remarried participants demonstrated a more positive health and well-being status [28,29]. However, the levels of SHS were high when positive attitudes towards remarriage were combined with participating in a friendship group in this current study. This finding could be explained by the traditional approach of the Korean elderly towards remarriage where the elderly often experience difficulties with step-families and legal issues [4,30]. Nevertheless, traditional age barriers could be removed if the attitudes towards remarriage were positive and combined with taking part in social gatherings. Furthermore, those who had negative attitudes towards learning reported their health as worse when they engaged in volunteering, compared with those who had negative attitudes towards learning without volunteering. This observation could be interpreted as personality types where people who appreciate learning also enjoy caring for and sharing with others, but the same is not true for their counterparts [31]. Thus, encouragement with volunteering by older adults who do not seek to learn could result in adverse effects. The same trend was not observed in the interaction between remarriage and the variables of AN, and friendship group and the variables of SA.
In summary, the notable finding of this study was that a positive perception of AN in learning and working, had a direct and positive influence on the SHS of older Korean adults. Moreover, engagement in volunteering and friendship groups were great moderators of positive AN in learning and remarriage respectively. Hence, encouragement of different types of SA, depending on the attitudes towards AN of older adults, would better contribute to enhancement of their SHS rather than a blanket application of an intervention for all the elderly adults. The practical implication of this would be to include survey questions for the elderly about their attitudes towards different types of SA and AN when they have their regular National Health Insurance medical check-up. This would identify an individual’s preference and enable the design of a well-matched health program. Overall, the findings of this study could add some insight to help policy proposals before introducing health promotions, by emphasizing the importance of understanding the perception of AN of the elderly, and its interplay with social participation.
There are some limitations to this study. The cross-sectional data did not allow causal relationships of the variables to be studied in temporal order, especially between social engagement and SHS. Nevertheless, this study assessed the prevailing attitudes towards AN and its interaction with SA among the Korean elderly (by which associations with their SHS could be identified). Regarding measurements, a single item was used to assess each variable which limited the study to capture the intended domain in a complete picture. Also, the level of involvement in the SA could not be compared among participants due to the data being collected using a dichotomous scale. A detailed assessment of the reliability and validity of the measurements was omitted since the study used national data. Further research may be conducted with different measurements to improve the accuracy of the findings. In addition, the scales to measure the variables of the data were developed based on the culture and situation of Korea. Thus, the generalizability of the measurements or the findings may be limited for other nations who are not experiencing “rapid aging” or not in an Asian culture. Further studies should use or develop more comprehensive measurements that can assess attitudes towards AN and SHS of the elderly under diverse circumstances.
Notes
Conflicts of Interest
No potential conflicts of interest relevant to this article.