Study of the Relationship Between Self-Efficacy, General Health and Burnout Among Iranian Health Workers
Article information
Abstract
Objectives
To evaluate the relationship between self-efficacy, general health and burnout of the staff at Shahroud University of Medical Sciences.
Methods
In 2015, 249 staff at Shahroud University of Medical Sciences (from a total reference population of 520 staff members) were selected through stratified random sampling. To collect the data, Sherer self-efficacy Scale, General Health Questionnaire and Maslach Burnout Inventory were used. The collected data were analyzed through ANOVA, Pearson correlation and Chi-square tests using SPSS 16. The relationship between self-efficacy, general health and burnout (latent factors) were studied using structural equation modeling with Stata 14.
Results
The mean age of participants was 36.97 ± 7.60 years, and the mean number of years work experience was 12.29 ± 7.57. The mean scores of general health, self-efficacy and burnout were 28.24 ± 11.14, 62.30 ± 9.21 and 81.67 ± 22.18, respectively. The results of the study showed a statistically significant relationship between self-efficacy and general health which equals −0.32. A statistically significant relationship also existed between burnout scores and general health scores (beta = 0.78).
Conclusion
The results showed that high self-efficacy improves the general health of employees at the Shahroud University of Medical Sciences and reduces burnout. Special attention should be paid to self-efficacy in the prevention of burnout.
Introduction
To succeed, organizations need healthy and self-efficacious employees [1]. Self-efficacy is an important factor for successful accomplishment of duties. Self-efficacy is a constructive mechanism by which the cognitive, social, emotional and behavioral skills of an individual are organized efficiently to achieve goals [1]. In the face of problems and surrounding issues, self-efficacy helps people to use their skills to achieve a good performance, and hence it creates or improves their sense of personal accomplishment, and consequently this enables general health [2]. General health is a major component contributing to overall well-being. The World Health Organization defined general health as “a state of well-being in which every person realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to contribute to her or his community.” [3].
To assess an individual’s general health status, the best questionnaire to use is the general health questionnaire with 28 items (GHQ-28). It assesses somatic symptoms, anxiety, insomnia, social dysfunction and severe depression [4]. One of the factors which affects general health is burnout which has 4 dimensions including emotional exhaustion, depersonalization, reduced personal accomplishment and conflict. Burnout develops gradually over time and may progress into a mental disorder [5]. A study has shown that employees who are at risk of burnout show poor job performance, and may face serious health problems over time [6]. Emotional exhaustion is a feeling of fatigue, and depletion of emotional resources which results from dealing with people [7]. Depersonalization refers to being impersonal or detached, and may result in negative or over reactions in certain situations, or detached treatment of other people in the work environment. Reduced personal accomplishment at work indicates a decline in the sense of competence and achievement in an individual, and it reflects low self-efficiency. A sharp decline in the quantity of health services has been reported when staff project a negative self-image and a negative attitude towards the job which results in a lack of communication with the patients [8]. Various factors lead to burnout such as the type of occupation, role conflict, heavy workload, management, lack of social support, organizational changes and competition, working hours, poor working conditions, perceived organizational inefficiencies, feeling of failure, low chance of promotion and strict laws and regulations [7,9,10]. The results of 1 study showed no relationship between sense of self-efficacy and job burnout [11], although some studies showed a relationship between feelings of self-efficacy and burnout [12,13]. Moreover, studies have demonstrated a relationship between burnout and general health [13–15]. A recent study of nurses showed that stress and self-efficacy, are the main related factors that are associated with job-related burnout [16]. Personnel of health care organizations are expected to be psychologically and physically healthy, so that they can perform their job roles well and provide a quality service to the public, thereby improving health.
Shahroud University of Medical Sciences in North East Iran is a large organization who employ many different professionals such as clinicians and support staff. This study was conducted to evaluate the relationship between self-efficacy, general health and burnout among the support staff of Shahroud University of Medical Sciences.
Materials and Methods
A cross-sectional study was conducted in 2015 in Shahroud University of Medical Sciences. There were 520 headquarter staff included in this study and stratified random sampling was applied to 50% of the staff using University Department personnel ID numbers (n = 249). There were 260 questionnaires distributed and the response rate was > 95%. After a brief explanation about the goals of the study and verbal informed consent was given, questionnaires were self-administered by the participants and completed in their own time. The proposal and methods of this study were reviewed and approved by the Ethics Committee of Islamic Azad University of Shahroud (Code no.: Ir. Iau.Shahrood. Rec1394.6).
In this study burnout, general health and self-efficacy were measured as latent variables. Other variables such as age, gender, education, work experience, marital status, satisfaction with income, essential life facilities and interest in the job were taken as correlated variables.
1. Measurement tools
The data collection instruments included a demographic questionnaire, Sherer self-efficacy scale, General Health Questionnaire with 28 items, (GHQ-28) and Maslach Burnout Inventory [7]. Sherer self-efficacy questionnaire includes 17 items which are scored on a 5-point Likert scale (strongly agree, agree, indifferent, disagree, and strongly disagree). Apart from items 1, 13, 8, 9, 3 and 15, other items are reverse items. Items 1–7 measure willingness to initiate behavior, items 8–13 measure willingness to expand effort, and items 14–17 measure persistence in the face of adversity. This scale has a maximum score of 85 and a minimum score of 17, and score of 58 and above indicates high efficacy, and scores less than 58 indicate low self-efficacy [17]. Barati reported a reliability coefficient of 70% for this scale in an Iranian population [18]. The General Health Scale includes 28 items which measure 4 subscales of somatic symptoms (items 1–7), anxiety/insomnia (items 8–14), social dysfunction (items 15–21), and severe depression (items 22–28). The scale is scored on a 4-point Likert scale ranging from 0 to 3 (0 = not at all, 1 = no more than usual, 2 = rather more than usual, 3 = much more than usual). For each person, 5 scores are calculated, 1 composite score for the whole scale and 4 subscale scores. The composite score can range from 0–84 and scores from the subscales can range from 0–21. Higher scores on each subscale are indicators of undesirable conditions. Scores lower than 6 indicate no health problems, while 7–11, 12–16 and 17–21 respectively indicate mild, average, and serious general health problems. Moreover, the composite scores of 0–21 indicate excellent health conditions, scores of 22–42 indicate good conditions, scores of 43–64 indicate average health conditions, and scores of 65–84 indicate poor health conditions. The cutoff point of 23 was determined for the scale (sensitivity of 70.5%, specificity of 92.3%, and overall classification error of 12.3%). Those who had a score of 23 or lower were classified as healthy people, and those who had a score of 24 and higher were suspected of having a health disorder. The Persian version of this scale has previously been reported to have a reliability coefficient of 0.89 for this questionnaire in Iranian people [19]. Maslach Burnout Inventory includes 25 items in 4 dimensions including emotional exhaustion, reduced personal accomplishment, depersonalization, and conflict. The inventory is scored on a scale including zero (never), 1 (several times a year), 2 (once a month), 3 (several time a month), 4 (once a week), 5 (several times a week) and 6 (every day). This inventory was validated in Iranian people [20]. Amiri et al [10,21] reported a reliability coefficient of 0.85.
The collected data were entered into SPSS 16.0 (SPSS Inc., Chicago, IL, USA) and analyzed through the Independent t test, Pearson correlation and Chi-square test. To study the relationship between 3 latent factors of self-efficacy, general health and burnout, structural equation modeling was used (Stata 14 software). In this model, responses are continuous and analyzed using linear regression models. The normality of variables was checked using the Kolmogorov–Smirnov test.
Results
In this study, 39.9% of the participants (n = 92) were males, 52.6% (n = 131) had less than 10 years of experience in the job, 79.2% (n = 197) had a bachelor’s degrees or higher, and 82.3% (n = 205) were married. The mean age of all the participants was 36.97 ± 7.60 years. The average work experience for all participants was 12.29 ± 7.57 years. The number of spouses’ who gained a bachelor’s degree or higher, was 130 (52.2%). Among the participants, 16.9% (n = 42) were satisfied with their income, 63.5% (n = 158) were partly satisfied, and 19.5% (n = 49) were dissatisfied. Moreover, 6.4% (n = 16) were slightly interested in their jobs, 21.7% (n = 54) were mildly interested, 52% (n = 130) were very interested, and 19.7% (n = 49) were extremely interested in their jobs. The mean scores of general health, self-efficacy and burnout and its subscales are presented in Table 1. Analysis of the data according to general health showed that 33.3% (n = 83) had a normal general health status, and 66.7% (n = 166) had adverse general health status (of those, 53% had a slight disorder, 12% had a moderate disorder, and 1.7% had an extreme disorder). There was a statistically significant relationship between general health and self-efficacy, such that people who had a normal general health, had higher mean self-efficacy scores (t = −5.95, p < 0.001).
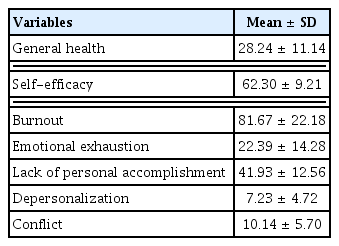
The mean scores of variables in the study sample.
In this study 71.9% had a high level of self-efficacy. The relationship between demographic variable and self-efficacy levels (low and high) is shown in Table 2. Analysis did not show a significant relationship between age, work experience, gender, education, marital status, income satisfaction, essential life facilities and interest in the job, and sense of self-efficacy (p ≥ 0.05; Table 2).

Relationship between demographic variables with self-efficacy.
The relationship between the demographic variable and general health status is shown in Table 3. Analysis using Chi-square showed no statistically significant relationships between age, work experience, education, marital status, satisfaction with income, essential life facilities and general health status (p ≥ 0.05; Table 3). However, a statistically significant relationship was observed between gender and general health status where men had a higher level of general health (p = 0.002). In this study, 12.4% of participants had a low level of burnout, and the frequency of moderate and high level of burnout were 80.7% and 6.8%, respectively. Using the Chi-square test no statistically significant relationship between age, gender, education, work experience, the essential facilities, job category and burnout were observed (p ≥ 0.05). However, a statistically significant relationship between marital status and overall burnout was observed using Chi-square analysis (p = 0.003) suggesting that high burnout was more common among married people. In addition, a statistically significant relationship was observed between the spouse’s job and burnout (p = 0.036). Moreover, a statistically significant relationship was observed between the spouse’s level of education and job burnout (p = 0.03), indicating that people whose spouses had a primary school education showed higher levels of burnout compared to other groups. A statistically significant relationship between overall satisfaction with income and burnout (p = 0.029) was observed using Chi-square analysis indicating that job burnout was higher in people who were dissatisfied with their income. Moreover, the relationship between a person’s interest in their job and overall burnout was statistically significant using Chi-square analysis (p = 0.001) indicating that high burnout decreased as the interest in the job increased (Table 4).
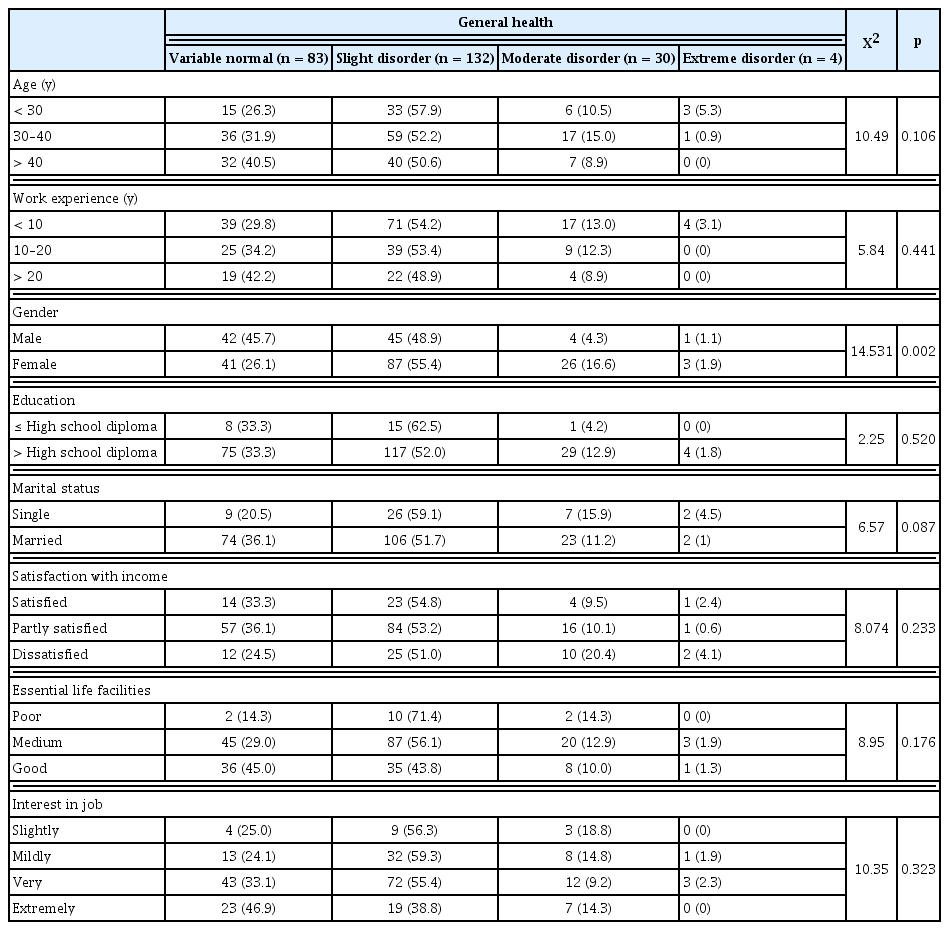
Relationship of demographic variables with general health.
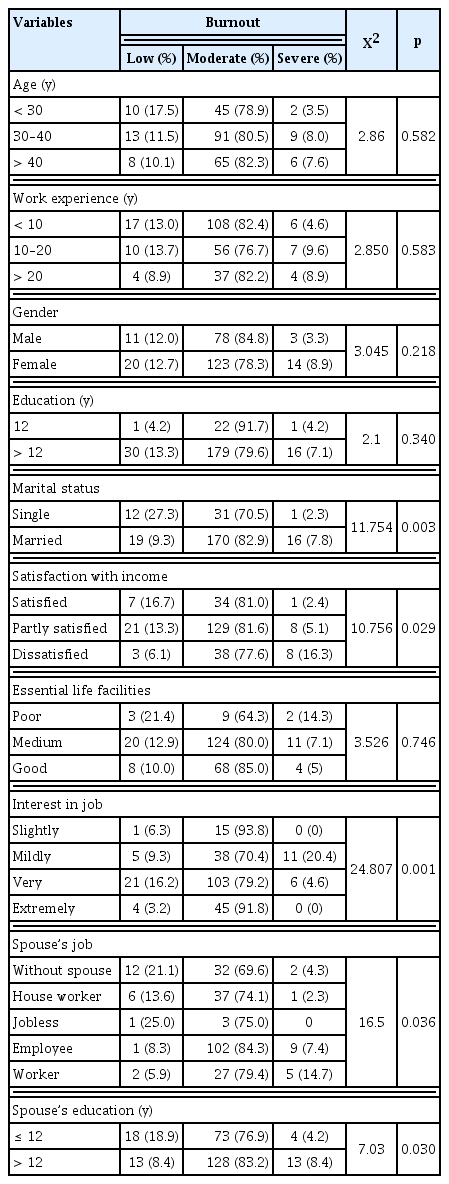
Relationship of demographic variables with burnout.
The Pearson correlation coefficients indicated statistically significant relationships between burnout and general health (r = 0.312, p = 0.001), and self-efficacy and general health (r = −0.37, p = 0.001). There was not a statistically significant correlation between burnout and self-efficacy (r = 0.11, p = 0.09).
Structural equation modeling of the relationship between the 3 latent variables of self-efficacy, general health, and burnout, showed that a statistically significant relationship existed between self-efficacy and general health (−0.32), indicating that an increase in self-efficacy would lead to a better level of general health (lower general health score). A statistically significant relationship also existed between burnout scores and general health scores, such that with an increase in burnout scores, general health scores also increased (β = 0.78) which indicated that people with burn out have a lower level of general health. The results also showed a negative correlation between self-efficacy and burnout score which was equal to −0.29 (Figure 1). This suggested that those who had high burnout scores had low self-efficacy scores. The likelihood test for model selection showed a statistically significant association (Chi-square = 204, p < 0.0001).
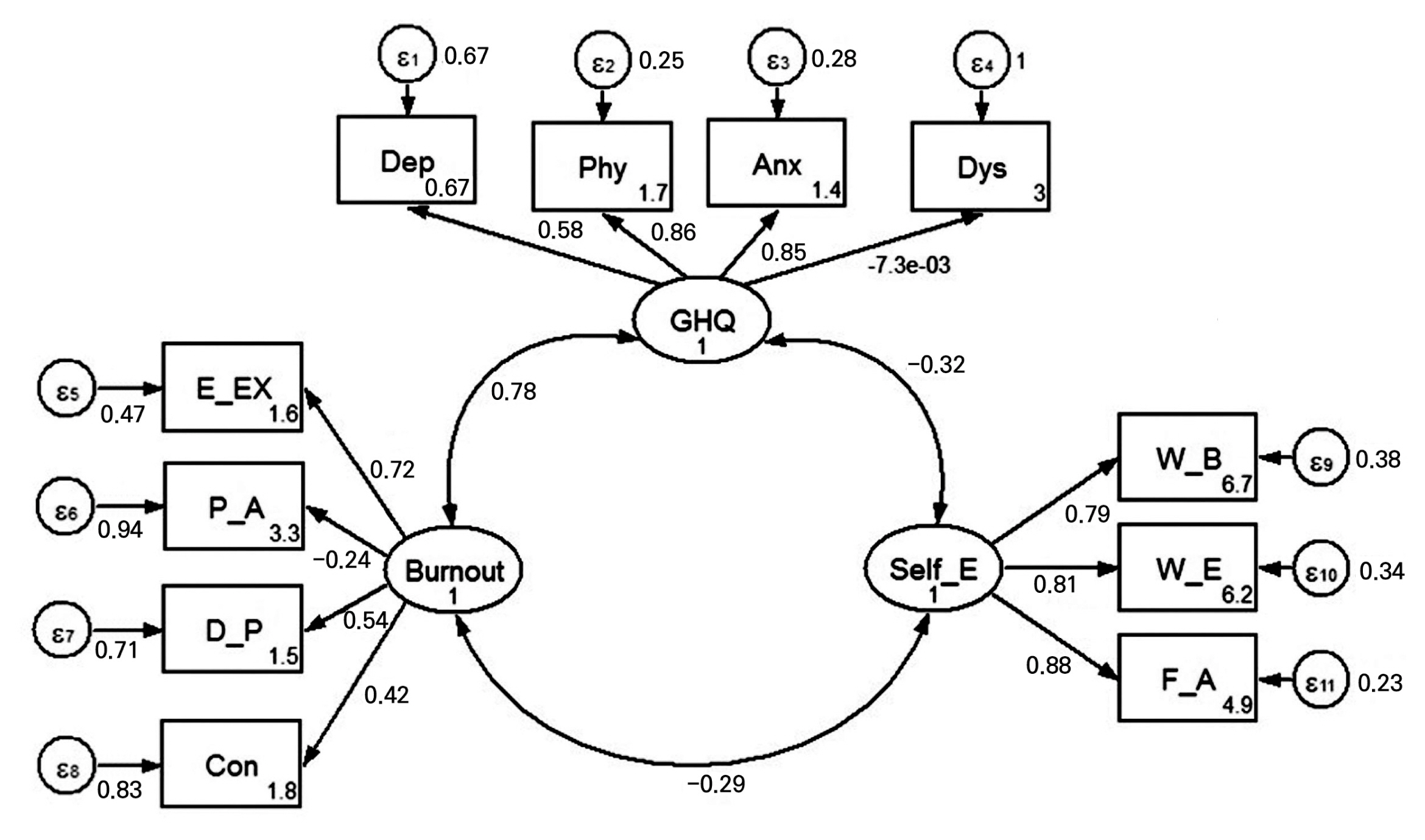
Association between self-efficacy, general health and burnout using a structural equation model.
W_B = willingness to initiate behavior; W_E = willingness to expand effort; F_A = face of adversity; Phy = somatic symptoms; Anx = anxiety/insomnia; Dys = social dysfunction; Dep = severe depression; E-EX = emotional exhaustion; P_A = reduced personal accomplishment; D_P = depersonalization; Con = conflict.
Discussion
The majority of participants had a high level of self-efficacy and 33.6% had a normal general health status. The high level of burnout was 6.8%, which was similar to a previous study of primary health care providers [10]. The results of this study showed that Shahroud University staff experienced less burnout than the other studies [22,23]. These variations can be related to population differences and diversity of the tasks performed by support staff.
Although the frequency of high emotional fatigue in participants 40 years and above was more than other age groups, no statistically significant relationship was observed between burnout and age groups, which is consistent with the results of 1 study [24], but not in line with other studies which reported a relationship between burnout and age [15,21,25]. There was not a statistically significant relationship between work experience and overall burnout, which tallied with some studies [10,12,24,25], but differed with other studies [15,20] which reported a statistically significant relationship between burnout and work experience. This can be explained by uniformity of work environment. The results of this study indicated that there was not a statistically significant relationship between gender and burnout.number of studies, but in line with the findings of Amiri and colleagues [10], Qarialavijeh et al [24] and Rashidi et al [25] who reported no relationship. However, in our study there was not relationship between gender and burnout but in contrast to this finding burnout has been described as a condition that predominantly affects women [12,26], and it can be related to psychological distress and psychosocial work factors [27].
There was a statistically significant relationship between marital status and job burnout which was in line with the results of some other studies [24,28], but not in line with the results of our previous study on primary health care providers [10]. The findings observed in this current study were based on univariate analysis, therefore the results may be affected by age and work experience. Therefore, these findings should be interpreted cautiously.
There were no associations between age as a predictor variable with the sense of self-efficacy, which is consistent with the results of Moghaddam et al [29], but inconsistent with the results of Mehdizadeh et al [30]. No statistically significant relationship was observed between the sense of self-efficacy with work experience. Aliyev and Tunc [12] reported no relationship between self-efficacy and work experience, which is consistent with the results observed in this current study. Lauermann and König [11] reported a negative relationship between self-efficacy and work experience which is not consistent with this current study. This finding may be related to identical and repeated tasks, and the lack of innovations in the working environment. Moghaddam and Poorahmad [29] reported that there was no relationship between gender and self-efficacy, which were in line with the findings of this current study, but it is inconsistent with the results of Aliyev and Tunc [12], Mehdizadeh et al [30], and Chamanabad et al [31]. This may be attributable to the uniformity of the work environment for male and females. In this current study, there was a negative relationship between self-efficacy and job burnout score, such that staff who were burned out had lower self-efficacy scores, and this finding was consistent with other studies [12,32,33]. In addition, the categorical analysis of data, showed no statistically significant relationship between burnout and self-efficacy, which is not consistent with the results of some studies [12,13,29,34] but it is in accordance with the study by Lauermann and König [11]. People with job burnout have a lower score for personal accomplishment and this can be related to other psychological variables such as self-esteem, which affects self-efficacy.
There was a statistically significant relationship between self-efficacy and general health, which is in line with the results of a number of studies on the relationship between self-efficacy and general health [31,35–39]. This current study showed that general health and burnout levels are significant predictors in the explanation of self-efficacy levels. This is due to the impact of psychological conditions on self-efficacy.
The relationship between general health and marital status was not statistically significant, which was inconsistent with the findings of Solhi et al [36], but is consistent with other studies [40,41]. A statistically significant relationship was observed between general health and gender, which was consistent with some studies [31,42]. It is thought that women are more subject to stress and psychological distress because the majority of women in Iran are bound to their social roles as housewives; even when women have salaried work outside the home.
There were statistically significant relationships between general health and burnout which was consistent with the result of a number of studies in Iran and in the world [13–15].
There are a limited number of studies which simultaneously measured 3 variables including self-efficacy, general health and burnout, and this was the most important limitation of this study. Many work-related and psychological factors that affect burnout are related to mental health. Some studies showed that management of work-related stress successfully improved job performance levels among nurses [43]. Observations of firefighters revealed that self-efficacy was a significant moderator of the relationships between perceived stress and burnout [44]. Another study showed that job self-efficacy related directly to job performance and psychological health several months later [45].
A limitation of this study was the restriction of the study population which included headquarters staff. The main strengths of this study were using valid questionnaires and sophisticated analytical methods.
Conclusion
The observations of this study showed that improvement in self-efficacy scores could improve general health status, and ultimately reduce staff burnout. Since 2/3 of the people had an adverse health status, paying attention to this, and implementing the necessary interventions may pave the way for providing a better health care service and lead to an improvement in public health. Special attention should be paid to self-efficacy when considering prevention of burnout in support staff.
Acknowledgments
The present article was extracted from the MSc thesis written by Seyed Reza Mirhoseini and was supported by Azad Shahrood University.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.