Perception and Practice of Road Safety among Medical Students, Mansoura, Egypt
Article information
Abstract
Objectives
To assess the knowledge and attitude of medical students towards road safety and to determine their driving behavior and its relation to different related factors.
Methods
This cross-sectional study involved 480 medical students at Mansoura University, Egypt. A self-administered questionnaire was used to collect student personal data, knowledge about road safety, attitude towards road safety, and driving practices.
Results
More than 40% of students experienced an injury in the previous year, mainly as a pedestrian (56%), and 15.2% practiced driving, although only 9.6% had a driving licence. Most of the students had correct road safety knowledge except for awareness that the safe time to read maps is when your vehicle is parked (44%), one should drive in the left lane (29.6%), and one should overtake from the right-hand lane only (25.8%). The majority of the students reported that road traffic injuries can be prevented (89.2%). The mean score of the driving practices of the students ranged from 0.66±1.04 to 2.44±6.28 and rural residents showed significantly higher score regarding errors and lapses.
Conclusion
Good road safety knowledge and a favorable, low risk attitude, did not translate into improved road traffic behavior and this highlights the importance of stricter implementation of the existing rules and including road safety in medical education programs.
Introduction
Currently, road traffic injuries are the 8th leading cause of death globally, and the principal cause of mortality in young people aged 15 years to29 years, and expected to be the 5th leading cause of death by 2030 unless urgent action is taken[1, 2].
The Global status report on road safety in 2015 showed that the highest road traffic fatality rates are in low or middle-income countries, which affect mainly pedestrians, cyclists, and users of motorized 2- or 3-wheeled vehicles [2]. In Eastern Mediterranean countries including Egypt, the estimated road traffic death rate is 19.9 per 100,000 populations in 2013 [2].
The main risk factors responsible for injuries are vehicles, human, road, and environmental [3]. Human practice is a main or contributory risk factor in 90% to 95% of road traffic injuries [4] as a result of speeding, the non-use of seatbelts, and distraction.
Recent reports reveal that nearly 1/3 of drivers in fatal crashes and 12% of drivers with serious injuries did not wear a seatbelt [5]. Speed has been described in different ways including driving over the speed limit, driving too fast for the weather conditions, or racing [6]. Younger drivers are more likely to be involved in fatal collisions as a result of distracted driving than adults [7].
According to Reason et al, [8] driver behaviors can be divided into 2 classes; errors and violations. This discrimination gave the basis for the development of the Manchester Driver Behavior Questionnaire (MDBQ) which showed that driver errors, violations, and lapses are 3 empirically distinctive classes of behavior. They stated errors as “the failure of planned actions to achieve their intended consequences”, violations as “deliberate deviations from those practices believed necessary to maintain the safe operation of a potentially hazardous system”, and lapses as “attention and memory failures”. Although errors and violations together are potentially hazardous and may cause a crash, violations were seen as deliberate behaviors. This English questionnaire has gained wide acceptance since its introduction in 2010, with 174 studies performed using this questionnaire or a modified version [9].
Medical students represent an important sector of the youth population. Being the doctors of the future, they have the responsibility of increasing awareness of the youth population about different healthy behaviors including road safety and, they will be responsible for emergency care. In Egypt, there has been no available research to assess drivers’ behavior in this important age group using MDBQ. This study aimed to assess the knowledge and attitude of medical students towards road safety and to describe their driving behavior (whether lapses, error, or violation), using MDBQ and its relation to different related factors.
Materials and Methods
1. Study location
This cross-sectional descriptive study was carried out in the Faculty of Medicine, Mansoura University during the period from November 2014 to March 2015. The target group was the students in all 6 grades which were subdivided into preclinical and clinical students. This study proposal was approved by both the Vice Dean of the Students’ Affairs and the Institutional Review Board of the Faculty of Medicine, Mansoura University.
2. Sample size
The sample size was calculated online (www.dssresearch.com). A pilot study was performed on 50 students and revealed that the prevalence of previous exposure to injuries in the last year was found to be 25%. The calculated sample size was equal to 480 with a 95% confidence level, and 80% study power.
A total of 550 questionnaires were distributed with a response rate of 87% [incomplete questionnaires (3.9%), lack of interest in the study (4.1%), and absence of some students during the study period (5%)].
3. Sampling technique
A stratified, cluster sampling technique was adopted. The students were selected from all 6 grades, with each grade considered as a stratum. From each stratum, 2 sections (clusters) were randomly chosen. All the students in the chosen clusters were included. The self-administered questionnaire was distributed during the practical sessions after being granted permission from the heads of departments. The authors gave brief explanations of the objectives and the method of filling out the questionnaire. Verbal oral consent was obtained from the students who were assured of their anonymity and the confidentiality of their responses. The investigators collected the completed questionnaires at the same session.
4. Instrument
The questionnaire was constructed after reviewing the relevant literature and it was divided into 4 parts (Table 1).

The items of the questionnaire used in this study.
5. Data analysis
The completed questionnaires were subjected to revision and the collected data were coded, processed and analyzed through SPSS (Statistical Package for Social Sciences Inc., Chicago, IL, USA, standard version release 16.0). A descriptive analysis of the collected data was performed in the form of frequencies, percent and mean ± SD. Chi-Square was used for testing significance of categorical data. For quantitative variables, Student t test was used to compare the means between different groups; 0.05 was chosen as the level of statistical significance. Exploratory factor analysis, with varimax rotation, was applied to the (MDBQ) data. The Kaiser-Meyer-Olkin value was 0.76. Results of Bartlett’s test of sphericity showed χ2=999.3 (df=325 p=0.000) and this demonstrated the suitability of the data for factor analysis.Principle component analysis was used as an extraction method. Eigenvalues above 1.00 were used, and based on these criteria 3 factors were identified. Factor loadings and screen plot were examined. Items were maintained if their factor loading was at ≥ 0.30. The internal consistency of the new factors was examined by using Cronbach α.
Results
This study involved 480 students, with a mean age of 20.2 ± 1.5 years, males representing 39.6%, 69.8% were urban residents, 45.8% were in the clinical phase of their studies, and 15.2% of the students practiced driving although only 9.6% had a driving licence. Less than half of the studied group (43.5%) were ever exposed to injuries, 41.7% were exposed to an injury in the previous year mainly as a pedestrian (56%), from which 46% needed medical care (data not shown in the tables).
Table 2 showed that nearly half of the students (46.9%) reported bad road conditions as an important cause of road traffic injuries, however only 11.7% reported that pedestrians’ lack of awareness of traffic regulations and laws was the cause. It was also found that clinical students showed significantly greater knowledge in all the mentioned causes of road traffic injuries than the preclinical students, but male students had significantly reported a car’s bad condition as a cause of road traffic injuries.

Knowledge of road safety measures according to gender and academic stage.
The students reported looking right and left and then walking the correct way for pedestrians to cross a road (56.2%) that was higher among preclinical students, followed by looking right, then left, and then right again, before walking (41.2%) which was significantly higher among clinical students.
A higher percent of students showed agreement to other road safety items, such as talking to the driver which reduces the drivers’ concentration (83.1%); this was significantly higher among preclinical and female students, cautious driving near schools (82.7%), safest way to use mobile phone while driving is use of hands-free devices (71.9%), one should wait patiently if pedestrians are taking too much time at the zebra crossing (71.5%) all the previous items were significantly higher among clinical students, loud music in the car can distract the driver (67.3%) that was significantly higher among female students, one should pull over when it is safe to give way to an ambulance with a flashing light (61.9%) in which clinical and male students showed significantly higher knowledge. However students’ awareness of some road safety measures is considerably low as safe time to read maps is when your vehicle is parked (44%) more among female and preclinical students, one should drive in the left lane (29.6%), and one should overtake from the right-hand lane only (25.8%) which was significantly higher among preclinical students.
The majority of the students mentioned that road traffic injuries could be prevented (89.2%), the use of mobile phones whilst driving increased the chances of an injury (72.1%), and riding a bicycle/motorbike without a helmet increased the chance of an injury (62.9%), and both the previous items were significantly higher among clinical students, driving a vehicle without a valid licence is an offense (67.9%), and that there was a less favorable attitude showed towards the insistence of passengers’ use of seatbelts (38.8%) which was significantly higher among preclinical than clinical students. The percentage of students that believed drivers were afraid of punishment so they used seat belts was 62.1%, and was significantly higher among male and clinical students, followed by drivers convinced of the importance of using seatbelts (24.6%) in which female and preclinical students showed a significantly better attitude. Less than half of the students (44%) thought that the use of seatbelts reduced the disabilities caused by road traffic injuries, with clinical students showing a significantly better attitude towards all the benefits of seatbelt use. Nearly the same percentage (44.2%) of students reported movement restriction as a reason for not using seatbelts. However, 57.7% felt convinced that seatbelt use was beneficial mainly among clinical students (Table 3).

The attitudes of students towards road safety measures according to gender and academic stage.
The mean score of the driving practices of the students ranged from 0.66 ± 1.04 (crossing a junction knowing that the traffic lights have already turned red) to 2.44 ± 6.28 (disregarding the speed limits late at night or early in the morning).The mean score for violation was insignificantly higher among male, rural residents, clinical students, and those without a driving licence. The rural residents showed significantly higher score regarding error and lapses, which were also higher among preclinical students and those who do not have a driving licence. Although there was no significant statistical difference in the mean scores of the 3 domains and exposure to injury, higher scores were found among those exposed to injuries (Table 4).

Behaviors and practices of the driver as measured by the Manchester Driver Behavior Questionnaire and its relationship to different related factors.
The overall results from the Exploratory Factor Analysis are presented in Table 5. The 3-factor solutions were responsible for 49.4% of the total variance. The items loadings ranged from 0.319 to 0.794. The majority of the loading was >0.50. Only one item failed to load which was “stay in a motorway lane that you know will be closed ahead until the last minute before forcing your way into the other lane”. The first subscale which included 9 items was named “errors” and is responsible for approximately 33.2% of the total variance. The reliability α=0.86. The 2nd subscale which included 9 items was named “violation” and is responsible for approximately 8.8% of the total variance. The reliability α=0.51. The 3rd subscale which included 9 items was named “lapses” and was responsible for approximately 7.4% of the total variance. The reliability α=0.79. Across loading was detected where “misread the signs and exit from the roundabout on the wrong road” and “forget where you left your car in the car park” which were related to lapses and “sound your horn to indicate your annoyance to another driver” which was related to violation, were loaded in the error subscale. “fail to notice that pedestrians are crossing when turning into a side street from a main road” which was related to errors, was loaded in the violation subscale. Also “attempt to overtake someone that you had not noticed to be signaling a left/right turn” which was related to errors, was loaded in the lapses subscale.
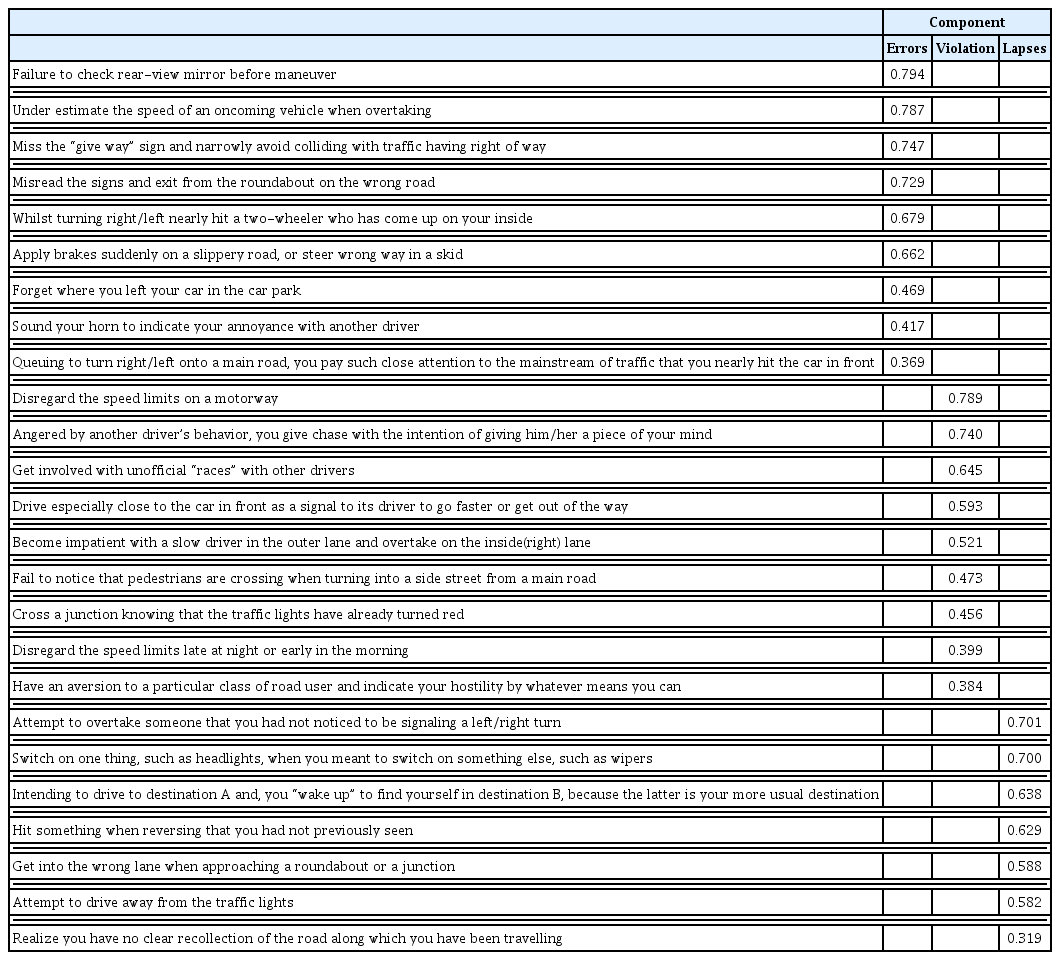
Exploratory factor analysis of the Manchester Driver Behavior Questionnaire.
Discussion
Young drivers are a vulnerable age group of drivers worldwide, with a significantly higher risk of being involved in a road traffic injury compared with other age groups of drivers [11].
In this study, it was found that the students who drive are much higher than those who have a driving licence. This shows a problem highlighting noncompliance with regulations and this attitude may be responsible for bad road behavior and injuries. In general, there was a small percentage of the students who practiced driving and this is in agreement with another Egyptian study [12], but differs from studies conducted in the United States [13] and in a South Indian state [14] where ≥70% of the students had cars and driving licences, reflecting the difference in socioeconomic status. At the same time about 40% were exposed to injury in the previous year, mainly as pedestrians. Lower rates (26.7% and 21.9%) were reported by 2 studies in Egypt amongst a similar target group, but the difference may be attributed to the time of exposure as they limited their questions to the previous 6 months only [12, 15]. Also, in Uttarakhand, 20% of the medical students previously experienced injuries [16].
Awareness about road safety is a very important step for road traffic injuries prevention; in this study, nearly half of the students reported bad road conditions as an important cause of road traffic injuries. In Malaysia [17] and in Trinidad [18], it has been reported that high speed and the noncompliance of drivers to road traffic regulations were the main causes of road traffic injuries. The better condition of their roads gives drivers the chance to drive at higher speeds in contrast to the roads in our locality. Students reported looking right and left and then crossing a road as a pedestrian, which was similar to that found in an Indian study [19], however, the correct procedure which is looking right, then left, and then right again, before walking, achieved (41.2%). Much higher rates were reported in Kenya (53.3%) [20], but only (3.09%) was found in India [19]. Correct student knowledge of other road safety items was recorded (60%–83%) as talking to the driver decreases the drivers’ concentration, being cautious whilst driving near schools, the safest way to use a mobile phone whilst driving is to use hands-free devices, patiently wait if pedestrians take too much time at the zebra crossing, loud music in the car can distract the driver, and one should pull over when it is safe to give way to an ambulance with a flashing light. However, these items were considerably low (≤ 35%) in an Indian study [14], whilst the students’ lack of awareness of traffic regulations was reported by others [17].Students’ awareness of some road safety measures was considerably low; a safe time to read maps is when your vehicle is parked (44%), one should drive in the left lane (29.6%), and one should overtake from the right-hand lane only (25.8%); this was in agreement with another study in India [14].
Despite the favorable attitude shown by the majority of the students who reported that road traffic injuries could be prevented, the use of seatbelts reduced the disabilities caused by Road traffic injuries and they felt convinced of its use but they believed that drivers were only using seatbelts because they were afraid of punishment. The same was reported by others [17]. However, in an Egyptian study [15], 78.6% of the total participants believed that road crashes were not preventable, but the reverse was observed regarding those exposed to injury. Most of the students believed that driving a vehicle without a valid licence was an offence and the use of mobile phones during driving, and riding a bicycle/motorbike without a helmet, increased the chances of an injury and these were in agreement with other studies [21, 22].
By examining the driving practices of students who drive using MDBQ, we found that the mean score of the driving practices of the students ranged from 0.66 ± 1.04 to 2.44 ± 6.28. This is in contrast to a study reported from Iran where much lower means were reported (0.443 ± 0.736 to 1.24 ± 1.072) [23]. The higher score observed in the study although of the high road safety related knowledge of the participants that was not reflected in their practice and also combined with those driving without license. Higher means were reported in Qatar (1.06 ± 1.31 to 2.25 ± 1.74) [24]. Gender was not significantly related to driver practices although males reported slightly fewer errors and more violations than females. The same was reported in other studies [7, 25]. Although the DBQ 3 domains were not significantly related to injury exposure, other studies reported that either violation alone [26] or both violation and errors [7] were significantly related to involvement in a crash in the previous year.
Unsafe driving practices as violations, lapses, and errors, may cause unpremeditated injuries among medical students. Despite their correct awareness of driving risks, improved driving behavior was not observed and this appeared also from the difference between driving and having a valid license. This highlights the importance of stricter implementation of the existing rules that may limit risky behaviors. At the same time, health education and training courses on road safety behaviors in the universities should be established.
1. Study limitations
This is a single-center study including a highly selective group of young adults; its results may not be representative of the similar age group in the national population.
2. Implications and contribution of the study
This study included a very important group of young adults because at their age, they are at the beginning of their driving experience, or because they are in the medical field who will be future doctors that can help others in their practices.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.