Prevalence of Internet Addiction, Poor Sleep Quality, and Depressive Symptoms Among Medical Students: A Cross-Sectional Study
Article information
Abstract
Objectives
This objective of the study was to report the prevalence of internet addiction, sleep quality, depression, anxiety, and stress in undergraduate medical students.
Methods
A cross-sectional, questionnaire-based study was conducted among 221 undergraduate medical students at Government Doon Medical College, Dehradun, Uttarakhand. Data pertaining to internet addiction, sleep quality, and depressive symptoms were also collected using validated and reliable questionnaires (Young Internet Addiction Test, Pittsburgh Sleep Quality Index, and Depression Anxiety Stress Scale 21).
Results
The prevalence of poor sleep quality, severe anxiety, and severe depression was 33.9%, 7.3% and 3.6%, respectively. The place of residence was significantly associated (p = 0.006) with internet addiction. The mean Young Internet Addiction Test score was higher in students residing in hostels compared with students staying with families. Stress was associated with age. The mean stress score was higher in the age group 17–20 compared with the 21–24 age group. Stress and depression were independent predictors of sleep quality.
Conclusion
Quality sleep is the key for good health. Based on limited samples, this study showed that poor sleep quality was associated with stress and depression. Hence, continuous counselling is suggested for supporting students managing their stress and depression.
Introduction
India is ranked as the second largest online market in the world, behind China with over 560 million internet users [1]. By 2021, it is predicted there will be over 600 million internet users in India; currently almost 71% of the internet users are men compared with 29% female [1].
Internet addiction has been described in terms of a loss of control in internet use [2], lack of time management and craving for the internet [3] and the cause of social problems [4]. The global prevalence of internet addiction among 3,651 medical students was reported as 30.1% [5]. Anxiety in 40,348 medical students globally was observed as 33.8% [6], and depression in 62,728 medical students globally was determined as 28% [7]. The use of internet is both beneficial and detrimental to the user’s health. Internet addiction has led to an increase in mental health disorders [8]. Internet addiction is not only affecting the quality and duration of sleep, it is also leading to a higher incidence of insomnia [9,10], psychiatric disorders such as depression, anxiety, alcohol addiction, and attention deficit in college students [11]. It has also negatively influenced the duration of bedtime sleep, caused daytime fatigue, and impaired work performance [12]. The internet has become a basic necessity in people’s lives leading to internet addiction which is associated with depression, poor sleep quality, severe mood changes, low self-esteem, impulsivity, suicide, lack of physical activity, and various health concerns including lifestyle disorders such as obesity, back pain, and migraine [13,14]. Internet addiction is a major contributor to anxiety and stress, impaired quality of life [15], lack of physical activity [16], trouble in communication and interaction with others in a healthy, positive, and meaningful way [17].
Sleep is the natural state for relaxation of mind and physical body, and it is also necessary for the secretion of adequate growth hormone required for the normal physical development in children and adolescents [18,19]. Internet addiction is rising among school and college students not only affecting sleep duration and quality, but also affecting the quality of work and concentration power. In a study conducted in 2015 in Vietnam, sleep disturbance and sleep quality were directly related to internet addiction in both young adults and adolescents, respectively [20]. Overnight use of smartphones in a study conducted in 815 young adults in Denmark 2013, reported that 12% used their phones 3–5 hours after the self-reported bedtime [21]. Sleep quality and sleep index can be measured using the Pittsburg sleep Quality Index (PSQI) to measure quality and duration of sleep in adults. It is used to differentiate sleep into “good” and “poor” sleep on the basis of 7 domains-sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medication, and day time dysfunction over the last month [22].
Studies have reported that female college students have poor sleep quality compared with male students [12,23]. Poor sleep quality can be due to female hormone changes during puberty or menstruation [24,25]. The relationship between sleep quality and internet addiction has been reported [12,18,20]. Sleep quality is severely affected in medical students due to high academic and clinical demands [26]. However, there are a lack of studies describing the prevalence, and relationship between internet addiction, sleep quality, depression, anxiety, and stress among medical students, so this study aimed to address these issues in medical students of Dehradun.
Material and Methods
A cross-sectional, questionnaire-based study was conducted among undergraduate medical students at Government Doon Medical College, Dehradun, Uttarakhand. The study was conducted during the period between October 2019 and December 2019. Taking 64% as the expected prevalence rate of poor sleep quality from a tertiary care teaching hospital in India [27], at a 95% confidence level, the required sample size was calculated to be 181 to yield a prevalence estimate with 7% precision. Taking into consideration a potential non-response rate estimated as 20%, a total of 221 students were recruited into the study. A pretested, validated, self-administered, structured questionnaire was used for data collection. The questionnaire was in English, containing questions to record socio-demographic characteristics such as name (optional), age, gender, details of current residence. Data pertaining to internet addiction, sleep quality and depressive symptoms were also collected using 3 validated and reliable questionnaires, namely (1) Young Internet Addiction Test (YIAT) [28,29] (2) PSQI [30,31] (3) Depression Anxiety Stress Scale 21 (DASS-21) [32]. Young Internet Addiction scale shows very good internal consistency with an alpha coefficient of 0.93 in an Indian population as reported by Goel et al [33]. A semi-structured questionnaire was distributed among the students and informed consent was taken. Data was collected from medical students until 221 responses were recorded. Students were provided with an explanation about the aims and objectives of the study before written informed consent was given. They were asked to respond to the questionnaire on a voluntary basis. Approval for this study was granted by the Ethics Committee of Government Doon Medical College, Dehradun (IEC/GDMC/2019/24).
Data were entered in Microsoft Excel and data cleaning included missing values and outlier before data was analyzed in SPSS Version 23.0 (IBM SPSS Statistics for Windows, Version 23.0. IBM Corp, Armonk, NY). Categorical data were reported in terms of numbers and percentages. Continuous data were summarized using the mean and standard deviation. To study the association between categorical variables, Chi-square test of association was used. To study differences in means with respect to categories, Analysis of Variance was used. A p < 0.05 was considered to be statistically significant. The multiple linear regression model was used to control for confounders.
Results
A total of 221 students’ data was included and analyzed in this study. There were 76.95% respondents (n = 170) who were females. Distribution of students was similar between the 2 categories of age (57.5% were 17–20 years and 42.5% were 21–24 years). The mean (± SD) age of respondents was 20.24 (± 1.51) years. Only a small percentage of respondents (18.6%) resided in a hostel, while the rest of the respondents (81.4%) were staying with their families (Table 1).
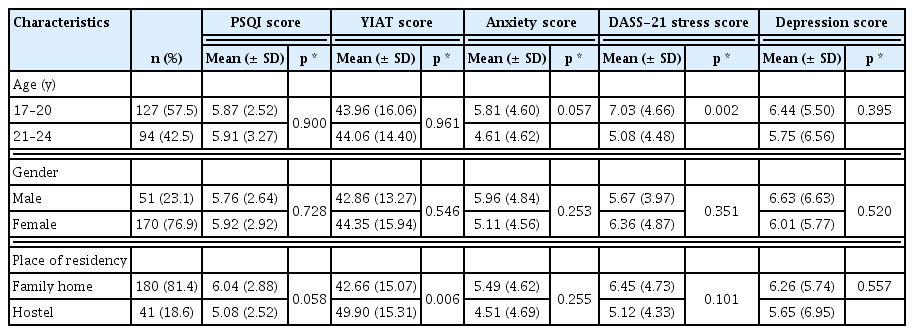
Demographic characteristics and comparison of mean scores of sleep quality, internet addiction and depressive symptoms.
It was determined that only 1.4% (n = 4) of students were suffering from moderate stress, and 4.5% (n = 10) students had mild stress. In this study, 67% (n = 149) participants had a YIAT score category of 20–39 points. There were 5.9% (n = 13) of respondents who potentially had an internet addiction whose score was between 70–100 points. There were 33.9% (n = 75) of participants who were determined to have a PSQI score greater than 5, and hence were suffering from a poor quality of sleep. Application of the DASS-21 questionnaire showed that 7.2% (n = 16), 9.0% (n = 20), and 3.6% (n = 8) of students had mild, moderate or severe depression, respectively. Similarly, prevalence of mild, moderate, and severe anxiety were 10.9% (n = 24), 7.7% (n = 17), and 7.3% (n = 16), respectively. Prevalence of stress was observed as mild in 4.5% (n = 10) students, 1.4% (n = 4) as moderate, and normal for 93.7% (n = 207) of students (Table 2).

Prevalence of internet addiction, poor sleep quality and depressive symptoms among medical students.
Mean scores of PSQI to determine sleep quality, YIAT to score internet addiction, DASS-21 to assess anxiety, stress, and depression were tested for probable association with the demographic characteristics under study. None of the demographic variables (age, gender, and residency) were determined to be significantly associated. An association between YIAT score and place of residence was significantly associated (p = 0.006) with internet addiction. The mean YIAT score was higher in those who resided in a hostel (49.90 ± 15.31) as compared with students staying with families (42.66 ± 15.07). Stress was determined to be associated with age (p = 0.002). The mean stress score was higher in the age group of 17–20 years (7.03 ± 4.66) compared with the age group of 21–24 years (5.08 ± 4.48; Table 1).
A correlation matrix of scores for perceived stress, internet addiction, depression, anxiety, and stress portrayed that sleep quality scores were positively correlated with stress, anxiety, and depression scores. A moderate positive significant correlation was determined between the PSQI score and DASS-21 scores for stress (r = 0.458, p < 0.001), depression (r = 0.428, p < 0.001) and anxiety (r = 0.395, p < 0.001), respectively. The correlation coefficient between YIAT and PSQI, stress, depression and anxiety were not determined to be statistically significant (Table 3).

Correlation matrix of sleep quality index and internet addiction with stress, depression, and anxiety.
After applying simple linear regression for sleep quality, DAS-21 scores for stress, depression and anxiety were determined to be significant predictors of sleep quality. Unadjusted regression coefficient of age, and YIAT score were determined not to be significant predictors of sleep quality. However, multiple linear regression revealed that stress, depression and anxiety were independent predictors of quality of sleep. The regression coefficient of stress and depression was 0.188 (p = 0.003), and 0.084 (p = 0.046), respectively. This indicated that for 1-unit increment in stress score, PSQI increased 0.188 times, while 1-unit increment in depression score resulted in an increment of 0.084 times. In a multivariate setting, age was not determined to be a statistically significant factor associated with sleep quality, and neither was internet addiction score (p = 0.777; Table 4).
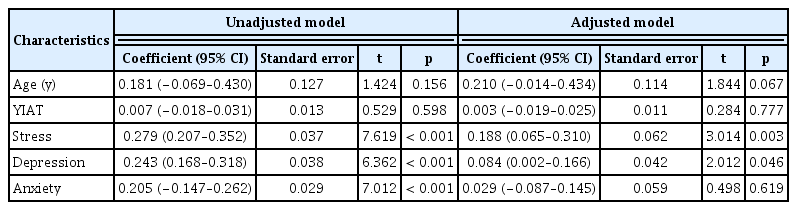
Results of multiple linear regression on factors associated with sleep quality.
Discussion
This study determined the prevalence of internet addiction, poor sleep quality, and depressive symptoms among medical students. The substantial findings of this study were the prevalence of severe anxiety and severe depression which occurred in 7.3% and 3.6% of students, respectively. The place of residence was significantly associated with internet addiction, where the mean YIAT score was higher in students who lived in a hostel compared with students staying at home with families. Stress was determined to be associated with age where the mean stress score was higher in the age group 17–20 years compared with the age group 21–24 years; stress and depression were independent predictors of sleep quality.
The results of this present study showed the majority of students had no problems with depression, anxiety, and stress, but they had unsatisfactory quality of sleep (overall global mean score of 5.88 (SD ± 2.85). There was no significant correlation of PSQI score with internet addiction which was consistent with the findings of another study conducted by Wolniczak et al [34], where the difference in mean PSQI score, and scores on its different components among undergraduate students (according to Facebook dependency) was reported. In line with the results from that study, no significant difference in total PSQI scores were observed in this study according to demographic charateristics.
PSQI scores were positively correlated with depression, anxiety, and stress in students, supporting previous findings regarding the relationship between sleep quality and depressive disorders [35]. Furthermore, societal and academic stress and demands disturb sleep, cultivating poor sleep quality [36]. So, to curtail the problem of depressive symptoms among medical students, the educational body can help the students by fine-tuning class hours with academic staff to recognize the functional need for sleep.
This present study reports that psychological disorders have a significant contribution to poor sleep quality index amongst medical students. Parallel results using DASS-21 have been described by Rezaei et al [37] where depression, anxiety, and some sleep hygiene behaviors were significantly associated with higher PSQI scores among pre-clinical medical students. A study conducted among Saudi Arabian medical students also reported that anxiety, stress, and depression had a significant impact on sleep quality.
There is a significant difference in anxiety and stress scores in terms of age. The higher age group in this current study had a greater mean value of depressive symptoms compared with the lower age group. Bhandariet al [38] reported that the age of older students was significantly associated with depressive symptoms.
This study’s finding suggests that there was no substantial effect of the use of the internet on sleep quality. Tao et al [39] reported that internet dependence was a multidimensional phenomenon due to having a wide variety of uses. To evaluate an estimated mean number of hours of internet use per day may be a crude measure. Medical students usually have a high academic load which will have a major contribution to psychological distress, which may affect sleep disorder. Longitudinal and interventional studies are needed to understand the causes and consequences of sleep disorder among medical students.
There are few studies in Uttarakhand state which have examined sleep habits of medical students; this study assessed the sleep quality and its associated factors. The association among psychological disorders (depression, anxiety, and stress), sleep quality, and internet addiction was explored. To the best of our knowledge, there are few cross-sectional studies that have examined the association among psychological distress, internet use, and sleep quality using standardized measures (DASS-21, YIAT, and PSQI) on medical student’s in Uttarakhand States.
There are limitations in this study including the cross-sectional methodology which limited the capacity of this study to measure sleep quality changes during academic activity, and prevented study of associated relationships between the confounding factors. Although this study dealt with only some potential demographic variables (age, sex, and residency), other variables are associated with depressive symptoms including socio economic status, behavioral variables (tobacco use, alcohol use, sexual activity), and educational variables (class hours, academic year, campus type, academic performance in previous year), that have not been considered in this study.
Conclusion
In this study almost one third of medical students reported poor sleep quality. Stress and depression were determined as independent predictors of sleep quality. However, because of the cross-sectional nature of this study, the causal mechanism behind this relation could not be determined. Further, longitudinal studies on larger sample sizes are required to understand this observation. Considering findings of this study, counseling sessions for anxiety, stress, and depression would seem appropriate.
Notes
Conflicts of Interest
The authors have no conflicts of interest to declare.