
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 14(3); 2023 > Article
-
Original Article
Vaccine effectiveness and the epidemiological characteristics of a COVID-19 outbreak in a tertiary hospital in Republic of Korea -
Seonhee Ahn1
 , Tae Jong Son1, Yoonsuk Jang1, Jihyun Choi2, Young Joon Park2, Jiseon Seong3, Hyun Hee Kwon4, Muk Ju Kim5, Donghyok Kwon6
, Tae Jong Son1, Yoonsuk Jang1, Jihyun Choi2, Young Joon Park2, Jiseon Seong3, Hyun Hee Kwon4, Muk Ju Kim5, Donghyok Kwon6 -
Osong Public Health and Research Perspectives 2023;14(3):188-196.
DOI: https://doi.org/10.24171/j.phrp.2023.0066
Published online: June 8, 2023
1Division of Infectious Disease Response, Gyeongbuk Regional Disease Response Center, Korea Disease Control and Prevention Agency, Daegu, Republic of Korea
2Epidemiological Investigation Team, Korea Disease Control and Prevention Agency, Cheongju, Republic of Korea
3Division of Infectious Disease Control, Daegu Metropolitan City Hall, Daegu, Republic of Korea
4Department of Internal Medicine, Daegu Catholic University School of Medicine, Daegu, Republic of Korea
5Department of Infectious Disease, Daegu Catholic University Medical Center, Daegu, Republic of Korea
6Division of Public Health Emergency Response Research, Korea Disease Control and Prevention Agency, Cheongju, Republic of Korea
- Corresponding author: Donghyok Kwon Division of Public Health Emergency Response Research, Korea Disease Control and Prevention Agency, 187 OsongSaengmyeong 2-ro, Osong-eup, Heungdeok-gu, Cheongju 28159, Republic of Korea E-mail: vethyok@korea.kr
© 2023 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 1,461 Views
- 72 Download
Abstract
-
Objectives
- Healthcare facilities are high-risk sites for infection. This study analyzed the epidemiological characteristics of a coronavirus disease 2019 (COVID-19) outbreak in a tertiary hospital after COVID-19 vaccination had been introduced in Republic of Korea. Vaccine effectiveness (VE) and shared anti-infection strategies are also assessed.
-
Methods
- The risk levels for 4,074 contacts were evaluated. The epidemiological characteristics of confirmed cases were evaluated using the chi-square test. The “1 minus relative risk” method was used to determine VE in preventing infection, progression to severe disease, and death. In the largest affected area (the 8th floor), a separate relative risk analysis was conducted. A multivariate logistic regression analysis (with 95% confidence interval [CIs]) was used to identify transmission risk factors with a significance level <10% via the backward elimination method.
-
Results
- In total, 181 cases of COVID-19 were confirmed, with an attack rate of 4.4%. Of those cases, 12.7% progressed to severe disease, and 8.3% died. In the cohort isolation area on the 8th floor, where 79.0% of the confirmed cases occurred, the adjusted odds ratio was 6.55 (95% CI, 2.99–14.33) and 2.19 (95% CI, 1.24–3.88) for caregivers and the unvaccinated group, respectively. VE analysis revealed that 85.8% of the cases that progressed to severe disease and 78.6% of the deaths could be prevented by administering a second vaccine.
-
Conclusion
- Caregiver training for infection prevention and control is necessary to reduce infection risk. Vaccination is an important intervention to reduce the risk of progression to severe disease and death.
- Patients with pneumonia of unknown cause in China on December 31, 2019, were subsequently identified as having severe acute respiratory syndrome coronavirus-2 [1−3]. Patients with confirmed coronavirus disease 2019 (COVID-19) exhibited symptoms of fever, cough, and respiratory distress 2 to 14 days after exposure to the pathogen [4]. With COVID-19 spreading worldwide, the World Health Organization declared COVID-19 a public health emergency of international concern on March 11, 2020.
- Since its first case was confirmed on January 20, 2020, Republic of Korea has achieved stable management of the COVID-19 pandemic using the 3T strategy (tracing, testing, and treatment) and social distancing measures [5].
- In Republic of Korea, 705,900 confirmed COVID-19 cases occurred between January 20, 2020, and January 19, 2022, with 10,882 (1.5%) related to outbreaks in healthcare facilities [6]. Despite robust infection control efforts, nosocomial COVID-19 outbreaks have been reported throughout the pandemic [7−10]. Studies have shown attack rates for nosocomial confirmed COVID-19 cases ranging from 15.5% to 30.9% [8,9]. In addition, hospitalized patients with nosocomial COVID-19 have an increased risk of prolonged hospitalization and death. Heightened public anxiety has resulted in a reluctance to go into healthcare facilities for treatments or diagnostic tests. This may account for the significant reduction in hospital admissions and likely contributed to the high mortality rates [7].
- Healthcare facilities are places where both patients and workers commuting from local communities are prone to infection [11−13]. Outbreaks in healthcare facilities burden local healthcare systems and pose a threat to public health because of the high risk of transmission to local communities [14−16].
- This study investigated a nosocomial COVID-19 outbreak in a tertiary hospital (hereinafter referred to as hospital A) located in Daegu Metropolitan City that involved 181 confirmed cases following the second round of vaccinations in Republic of Korea. Hospital A had 874 beds and admitted 70 to 100 patients daily. In this 15-story building with 2 underground levels, floors 5 to 14 were inpatient wards, and 1 ward on the 14th floor was operated strictly for COVID-19 isolation. The 8th floor included oncology and internal medicine (ward 1) and 2 orthopedic wards (wards 2 and 3). Although separated by department, patients and caregivers moved between wards, depending on bed availability. This study analyzed the epidemiological characteristics, transmission risk factors, vaccine effectiveness (VE), and response strategies of a nosocomial COVID-19 outbreak in a tertiary hospital.
Introduction
- Case Definitions
- • Caregiver: A caregiver association member who provides care and support for a patient with COVID-19.
- • Family caregiver: A family member who provides care and support for a patient with COVID-19.
- • Healthcare worker (HCW): Anyone working in a hospital setting.
- • Severe disease: The stage of COVID-19 for which patients are treated with high-flow oxygen therapy, mechanical ventilation, extracorporeal membrane oxygenation, or continuous renal replacement.
- • Unvaccinated: A person who has not received a vaccine or is within 14 days after their first ChAdOx1 nCoV-19 (AstraZeneca), BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna), or Ad26.COV2.S (Janssen/Johnson & Johnson) vaccine.
- • Vaccinated: A person who is at least 14 days past their first vaccine (exception: Ad26.COV2.S).
- • Partially vaccinated: 1–14 days after a second vaccination.
- • Fully vaccinated: Completed 2 doses of vaccination; 14 days after a second vaccination with a ChAdOx1 nCoV-19, BNT162b2, or mRNA-1273, vaccine or 14 days after the first vaccination with an Ad26.COV2.S vaccine.
- Field Epidemiological Investigation
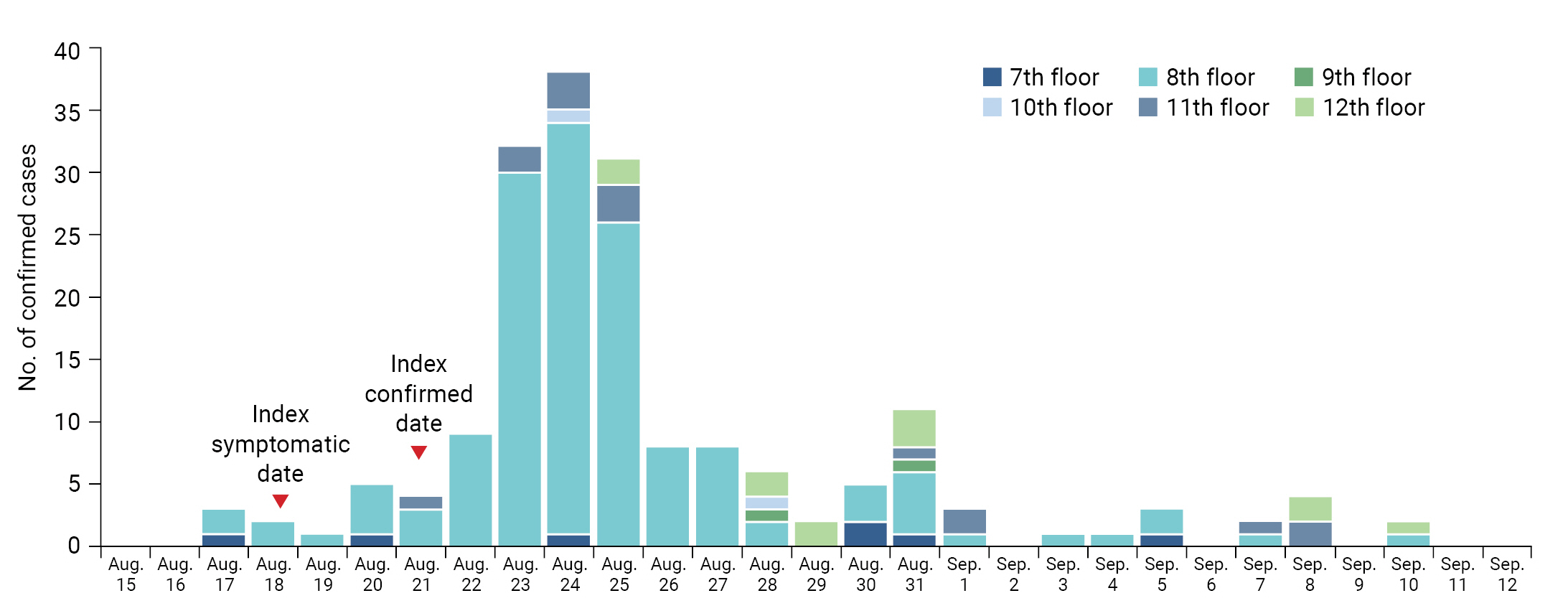
- Herein, we describe the response strategies to a nosocomial COVID-19 outbreak in a tertiary hospital that occurred from August 21, 2021 to September 10, 2021, as well as an analysis of the infection risk factors and VE. The index patient was a 49-year-old woman who worked as a caregiver in ward 1 (8th floor). She began showing symptoms (runny nose, headache, and dizziness) on August 18, 2021, was tested for COVID-19 on August 20, and was confirmed positive on August 21. After identification of the index patient, 9 patients in ward 1 tested positive for COVID-19 on August 22 during ward-wide testing, confirming the incident as a nosocomial outbreak. On August 23, another 18 confirmed cases were added after testing the contacts of the confirmed cases on the 8th floor, including patients from ward 3.
- A joint meeting of the hospital, public health center, city hall, and the Korea Disease Control and Prevention Agency (KDCA) evaluated the ongoing situation and discussed countermeasures. By August 23, a total 28 confirmed cases had been reported, including HCWs and caregivers. Many of the confirmed cases had not worn masks appropriately, and had moved across all floors in the hospital, from the basement to the 14th floor. Furthermore, since there were 3 confirmed cases (1 caregiver, 2 family caregiver) with a symptom onset date of August 17 (prior to the index case), the exposure period in the hospital was lengthened, indicating that many people had been exposed for an extended period of time. Therefore, those who were exposed in the hospital as of August 15 were considered contacts. A decision was made to test all 4,074 contacts within the hospital (1,232 patients, 288 family caregivers, 113 caregivers, and 2,441 HCWs). A field epidemiological investigation was conducted from August 24 to 27, 2021, and monitoring for new cases was continued until September 24, 2021.
- We investigated each contact’s sex, age, vaccination record, and exposure location (workplace for workers and caregivers, departments and rooms for patients and family caregivers). The risk levels were categorized as high, medium, or low based on the intensity of the contact’s exposure to confirmed cases (Table S1).
- Statistical Analysis
- All 4,074 contacts in hospital A were regularly tested until 14 days after the last confirmed COVID-19 case. Attack rates were calculated by sex, age, contact status, and exposure location. Data were analyzed using the chi-square test with the significance level set at p<0.05. Severity was calculated by tracing the confirmed cases that led to severe disease or death. The results were then used to calculate the VE in preventing infection, progression to severe disease, and death using the formulae: 1–(vaccination rate/non-vaccination rate)×100, 1–(rate of progression to severe disease among the vaccinated/rate of progression to severe disease among the unvaccinated)×100, and 1–(fatality rate among the vaccinated/fatality rate among the unvaccinated)×100, respectively, based on a 95% confidence interval (CI). In addition, an epidemic curve was created based on the date of symptom onset (confirmation date in asymptomatic cases) and location.
- The relative risk (RR) by sex, age, contact status, and vaccination record was analyzed (95% CI) to identify the transmission risk factors and evaluate their interrelatedness in all 430 contacts on the 8th floor where the index case occurred. Odds ratios (ORs) and 95% CIs were calculated, with statistical significance set at p<0.05, by performing multivariate logistic regression analysis using the backward elimination method for variables with a significance level <10%. SPSS ver. 18.0 (SPSS Inc.), and Microsoft Excel 2016 were used for statistical analysis and to create the epidemic curve.
- Ethics Approval
- Data were collected as part of the public health response to COVID-19 after obtaining a review exemption from the Institutional Review Board (IRB) of the KDCA (IRB No: 2022-09-01-PE-A). Informed consent was not required.
Materials and Methods
- Infection Control Strategies
- This event was a nosocomial outbreak that occurred in a tertiary hospital, where 181 cases were confirmed positive on the 8th floor (n=143) and other floors (n=38). The exposure period was August 15, 2021 (2 days before symptom onset on August 17), to September 10, 2021, when the last confirmed case occurred (Figure 1). Confirmed cases requiring intensive care were isolated in a dedicated ward of the hospital for ongoing treatment and those with milder symptoms were rapidly transferred to designated COVID-19 healthcare facilities. High-intensity and medium-intensity contacts were screened with polymerase chain reaction (PCR) testing at 3-day intervals (Table S1). Caregivers and HCWs (including interns and residents on rotation) were prohibited from taking business trips, vacations, and changing workplaces. New hospitalizations and visits were restricted until monitoring of the cohort isolation area was completed. Caregivers and HCWs in high-risk contact areas were provided with level D personal protective equipment, and mobile negative-pressure machines were put in the staff locker rooms. To prevent infection, Ad26.COV2.S vaccination was recommended for unimmunized individuals in the low-risk group. After obtaining consent, the initial doses were administered.
- Epidemiological Characteristics
- Of the 181 confirmed cases, 63.5% (n=115) were women, 54.7% (n=99) were aged ≥60 years, and those most frequently infected (47.0%, n=85) were patients, followed by family caregivers (21.5%, n=39), HCWs (18.8%, n=34), and caregivers (12.7%, n=23). The outbreak started with patients and family caregivers, then spread to caregivers and HCWs, and most confirmed cases occurred on the 8th floor (79.0%, n=143), where the index case occurred (Table 1).
- Although the overall attack rate was 4.4% (181/4,074), the attack rate was significantly higher (33.3%, 143/430) in the cohort isolation area (8th floor). Confirmed cases occurred in all wards, except in 5 single-occupancy rooms (total: 31 rooms, 22 multi- and 9 single-occupancy) (Table 1). The rate of progression to severe disease was 12.7% (n=23), and the fatality rate was 8.3% (n=15) (Table 2).
- Initial Symptoms
- Among the 181 confirmed cases, 59.7% (n=108) had symptoms (or exacerbated symptoms), including fever (45.4%), cough (45.4%), sore throat (38.9%), headache (29.6%), and phlegm (27.8%). In total, 40.3% (n=73) were asymptomatic, and the percentage of asymptomatic cases was lower on the 8th floor than on the other floors (36.4% vs. 55.3%, respectively) (Table 2).
- Vaccine Effectiveness
- Regarding COVID-19 vaccination, 45.3% (n=82) were unvaccinated, 19.3% (n=35) were partially vaccinated (1 dose), and 35.4% (n=64) were fully vaccinated (2 doses) (Table 1). The fully vaccinated rate by contact status was 20.0% for patients, 7.7% for family caregivers, 73.9% for caregivers, and 79.4% for HCWs.
- Compared with the unvaccinated group, the infection rate was reduced by 58.0% and 66.8% in the vaccinated and fully vaccinated groups, respectively. The rates of progression to severe disease were reduced by 77.0% and 85.8%, and the fatality rates were reduced by 79.3% and 78.6%, respectively. The VE for reducing infection rates, progression to severe disease, and fatality was statistically significant in both the partially and fully vaccinated groups (3).
- Risk Factors for the 8th-Floor Cohort Isolation Area
- The RR was calculated to evaluate the risk factors for infection in the 8th-floor cohort area where 79.0% of all confirmed cases occurred. By contact status, compared with HCWs, the RR was 3.50 (95% CI, 2.23–5.48), 2.70 (95% CI, 1.75–4.18), and 2.27 (95% CI, 1.51–3.41) for caregivers, family caregivers, and patients, respectively. By vaccination status, compared with the fully vaccinated group, the RR was 1.93 (95% CI, 1.44–2.59) and 1.68 (95% CI, 1.14–2.47) in the unvaccinated and partially vaccinated groups, respectively (Table S2).
- Multivariate logistic regression analysis was performed on variables with p<0.1 (i.e., contact and vaccination status), to determine the statistical significance of intergroup differences. Compared with HCWs, the adjusted ORs (aORs) were 6.55 (95% CI, 2.99–14.33), 2.42 (95% CI, 1.14–5.16), and 2.04 (95% CI, 1.09–3.82), in caregivers, family caregivers, and patients, respectively. In addition, the aOR was 2.19 (95% CI, 1.24–3.88) in the unvaccinated group compared with the fully vaccinated group, demonstrating statistically significant intergroup differences (Table 4).
Results
- This study described the response strategies in a COVID-19 outbreak in a tertiary hospital where 181 confirmed cases occurred over a period of 25 days. We also analyzed the risk factors for infection and VE.
- On August 23, 2021, a confirmed case of COVID-19 was identified, with symptom onset earlier than the index case. Furthermore, an additional confirmed case occurred in a ward via transfer from the ward where the index patient occurred. The possibility of exposure throughout the hospital could not be ruled out because various facilities in the hospital remained in use for several days, with many people in contact with each other. Therefore, PCR tests were conducted on all contacts (n=4,074) for 2 days (August 24–25), which led to the confirmation of 82 additional cases.
- Given that asymptomatic carriers can transmit COVID-19, when multiple confirmed cases occur in a facility vulnerable to infection, such as a healthcare facility, prioritizing the testing of all relevant contacts in the early screening of symptomatic cases can be an important intervention to prevent a large-scale nosocomial outbreak [17].
- In this study, asymptomatic cases accounted for 36.4% (52/143) of all cases on the 8th floor, and 55.3% (21/38) on other floors. Confirmed cases on other floors were identified in the hospital-wide testing implemented after multiple confirmed cases had occurred on the 8th floor. The early identification and isolation of confirmed cases during the initial stage of viral spread reduced the risk of additional transmission by asymptomatic COVID-19 carriers. This was also verified by the proportion of patients among the confirmed cases (43.4%, 62/143) on the 8th floor and (60.5%, 23/38) on other floors. While additional COVID-19 cases were identified on the 8th floor by testing close contacts of the infected, the confirmed cases on other floors were identified through hospital-wide testing, demonstrating that further spread can be forestalled in the early stage of an outbreak.
- In a large-scale outbreak, testing all relevant people makes it possible to implement self-quarantine of close contacts at an early stage. In this report, caregivers and HCWs who were close contacts self-quarantined, regardless of symptom status, and those in the low-risk group took over their roles. Quarantine of caregivers and HCWs may lead to insufficient patient care and work overload caused by the temporary personnel shortage. However, it is crucial to implement quarantine and place work restrictions on close contacts, whether symptomatic or asymptomatic, to reduce additional viral transmission [17]. In this case, early detection through hospital-wide testing and quarantine of confirmed cases and contacts was an important management strategy that ended an outbreak in a relatively short period.
- During the outbreak, caregivers were at high risk of infection due to their close contact with patients needing nursing care and help with activities of daily living. The results of multivariate regression analysis showed that they had a higher RR than other contact status groups. In addition, caregivers do not receive regular education on infection prevention and control [18]. Their insufficient knowledge of infection management and personal hygiene rules makes them more vulnerable to infection than other healthcare professionals [19]. However, this is not a new issue. In the 2015 Middle East respiratory syndrome coronavirus epidemic, 40% of confirmed cases were family caregivers and caregivers [20,21]. During the COVID-19 pandemic, however, hospitals in large-scale outbreak areas in Republic of Korea requested that family caregivers and caregivers submit a COVID-19 PCR-negative certificate within 72 hours or undergo periodic testing. The restriction that only 1 family caregiver or visitor was allowed to enter was also strictly followed. However, hospitals in regions with a relatively low number of confirmed cases, including hospital A, only required a COVID-19 PCR-negative certificate from patients within 72 hours before hospitalization. There were no access controls or restrictions on the number of family caregivers and caregivers.
- After the outbreak, hospital A limited caregivers (family or otherwise) to 1 person as much as possible and issued access approval cards, which required proof of a PCR-negative test within 72 hours prior to entering the hospital and allowed access only to the concerned area. In addition, body temperature was checked daily, and PCR testing was administered weekly for every person in the facility. Although this was a labor- and resource-intensive intervention, it was more effective than other caregiver education interventions (e.g., mandatory infection control programs) for preventing infection in the short-term [22,23]. This approach is recommended for high-risk facilities vulnerable to infection, including hospitals and long-term care facilities characterized by frequent close contacts, crowding, and confinement.
- The present study demonstrated a VE for preventing transmission of 66.8% in those who were fully vaccinated. Therefore, caregivers must be vaccinated. Caregiver education should also include information on how and when to wash hands, the chain of infection, how to use personal protective equipment, and recognizing signs of infection [24,25].
- Immediately after the development of COVID-19 vaccines in November 2020, worldwide vaccination began with high-risk population groups. In Republic of Korea, vaccinations began on February 26, 2021, with persons under 65 years of age living or working at long-term care facilities, HCWs in hospitals, and disinfection workers [26]. Vaccination of those over 65 years of age began on May 27, 2021.
- The outbreak described here occurred during the Delta variant wave of COVID-19. The fatality rate in hospital A was 8.3%., which was higher than the national average of 0.78% during the same period [27]. Furthermore, the VE against progression to severe disease and death was lower than the 1-year national average (93% and 95%, respectively) found in a related study of adults ≥18 years from February to September 2021 [28]. This was presumably due to the high percentage of patients with underlying diseases and those in the vulnerable age group (≥60 years) in hospital A.
- Nevertheless, the high VE in preventing progression to severe disease and death (85.8% and 78.6%, respectively) in the fully vaccinated group compared with the unvaccinated group, shows that vaccination is essential in high-risk facilities during respiratory infectious disease epidemics such as COVID-19.
Discussion
- The VE evaluation in this report was performed before the introduction of COVID-19 booster shots in Republic of Korea; thus there are no results on the effect of the booster. A limitation of this study was the inability to analyze the VE according to the interval between the vaccination date to the confirmation of infection. Therefore, if the corresponding data become available, further research is needed.
- Although it was impossible to completely block the influx of COVID-19 into hospitals, this study demonstrated that, once an outbreak occurred, information sharing and a joint response of the hospital, local government, and public health authorities, along with quick classification and quarantine of all contacts and routine testing for the early detection of confirmed cases, were essential interventions for early termination of the outbreak. In addition, to prevent transmission, infection prevention and control education is required for caregivers at healthcare facilities, and close contacts must be quarantined during the incubation period. Finally, vaccination is the most important measure to prevent infection and transmission, and to reduce the risk of progression to severe disease and death.
Conclusion
- • In an outbreak with 181 confirmed cases of COVID-19, the attack rate was 4.4%, 12.7% of cases progressed to severe disease, and the fatality rate was 8.3%.
- • Periodic testing for early detection of confirmed cases and the swift identification and quarantine of contacts were necessary measures for the early termination of a nosocomial outbreak.
- • This study provides relevant evidence-based findings that support vaccination as the most important measure to reduce the risk of progression to severe disease (by 85.8%) and death (by 78.6%).
- • To prevent transmission, ongoing infection prevention and control education is required for caregivers at healthcare facilities.
HIGHLIGHTS
Supplementary Material
-
Ethics Approval
Obtaining informed consent was exempted by the IRB of the KDCA (IRB No: 2022-09-01-PE-A) as no personal information was included in the study.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
-
Authors’ Contributions
Conceptualization: DK, YJP, TJS; Data curation: SA, JS, MJK; Formal analysis: SA, YJ, JC; Methodology: YJP, HHK; Project administration: DK; Visualization: JC; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Additional Contributions
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the KDCA or the institutions with which the authors are affiliated.
Article information

| Characteristic | Contact | Confirmed case (%) | Attack rate | pa) |
|---|---|---|---|---|
| Total | 4,074 | 181 (100.0) | 4.4 | |
| Sex | 0.937 | |||
| Male | 1,471 | 66 (36.5) | 4.5 | |
| Female | 2,603 | 115 (63.5) | 4.4 | |
| Age group (y) | <0.001*** | |||
| 0–19 | 79 | 2 (1.1) | 2.5 | |
| 20–39 | 1,607 | 31 (17.1) | 1.9 | |
| 40–59 | 1,295 | 49 (27.1) | 3.8 | |
| ≥60 | 1,093 | 99 (54.7) | 9.1 | |
| Exposure location (floor) | <0.001*** | |||
| 7th | 374 | 7 (3.9) | 1.9 | |
| 8th | 430 | 143 (79.0) | 33.3 | |
| 9th | 302 | 2 (1.1) | 0.7 | |
| 10th | 229 | 2 (1.1) | 0.9 | |
| 11th | 374 | 16 (8.8) | 4.3 | |
| 12th | 215 | 11 (6.1) | 5.1 | |
| Othersb) | 2,150 | 0 (0) | 0.0 | |
| Contact status | <0.001*** | |||
| Patients | 1,232 | 85 (47.0) | 6.9 | |
| Family caregivers | 288 | 39 (21.5) | 13.5 | |
| Caregivers | 113 | 23 (12.7) | 20.4 | |
| Healthcare workers | 2,441 | 34 (18.8) | 1.4 | |
| Vaccination statusc) | <0.001*** | |||
| Unvaccinated | 1,051 | 82 (45.3) | 7.8 | |
| Partially vaccinated | 553 | 35 (19.3) | 6.3 | |
| Fully vaccinated | 2,470 | 64 (35.4) | 2.6 |
| Characteristic | Total (n=181) | 8th floor (n=143) | Other floors (n=38) |
|---|---|---|---|
| Symptom | |||
| Symptomatic | 108 (59.7) | 91 (63.6) | 17 (44.7) |
| Fever | 49 (45.4) | 36 (39.6) | 13 (76.5) |
| Cough | 49 (45.4) | 40 (44.0) | 9 (52.9) |
| Sore throat | 42 (38.9) | 37 (40.7) | 5 (29.4) |
| Headache | 32 (29.6) | 27 (29.7) | 5 (29.4) |
| Phlegm | 30 (27.8) | 21 (23.1) | 9 (52.9) |
| Muscle pain | 24 (22.2) | 20 (22.0) | 4 (23.5) |
| Chills | 17 (15.7) | 13 (14.3) | 4 (23.5) |
| Shortness of breath | 8 (7.4) | 8 (8.8) | 0 (0) |
| Runny nose | 7 (6.5) | 6 (6.6) | 1 (5.9) |
| Pneumonia | 4 (3.7) | 1 (1.1) | 3 (17.6) |
| Loss of taste | 3 (2.8) | 2 (2.2) | 1 (5.9) |
| Loss of smell | 1 (0.9) | 1 (1.1) | 0 (0) |
| Othera) | 5 (4.6) | 5 (5.5) | 0 (0) |
| Asymptomatic | 73 (40.3) | 52 (36.4) | 21 (55.3) |
| Severity | |||
| Mild | 143 (79.0) | 116 (81.1) | 27 (71.1) |
| Severe disease | 23 (12.7) | 16 (11.2) | 7 (18.4) |
| Death | 15 (8.3) | 11 (7.7) | 4 (10.5) |
| Variable | Confirmed case | Total | RR (95% CI) | VE (1–RR)×100 (%) | p | |
|---|---|---|---|---|---|---|
| Infection | ||||||
| Unvaccinated | 82 | 1,051 | Reference | |||
| Vaccinateda) | 99 | 3,023 | 0.420 (0.316–0.558) | 58.0 | <0.001*** | |
| Partially vaccinated | 35 | 553 | 0.811 (0.554–1.189) | 18.9 | 0.328 | |
| Fully vaccinated | 64 | 2,470 | 0.332 (0.241–0.457) | 66.8 | <0.001*** | |
| Severe disease | ||||||
| Unvaccinated | 18 | 82 | Reference | |||
| Vaccinateda) | 5 | 99 | 0.230 (0.089–0.593) | 77.0 | 0.002** | |
| Partially vaccinated | 3 | 35 | 0.390 (0.123–1.241) | 61.0 | 0.143 | |
| Fully vaccinated | 2 | 64 | 0.142 (0.034–0.591) | 85.8 | 0.002** | |
| Death | ||||||
| Unvaccinated | 12 | 82 | Reference | |||
| Vaccinateda) | 3 | 99 | 0.207 (0.060–0.709) | 79.3 | 0.011* | |
| Partially vaccinated | 1 | 35 | 0.195 (0.026–1.444) | 80.5 | 0.125 | |
| Fully vaccinated | 2 | 64 | 0.214 (0.050–0.920) | 78.6 | 0.039* | |
| Variable | Adjusted odds ratio (95% CI)a) | p |
|---|---|---|
| Contact status | ||
| Patients | 2.04 (1.09–3.82) | 0.026* |
| Family caregivers | 2.42 (1.14–5.16) | 0.022* |
| Caregivers | 6.55 (2.99–14.33) | <0.001*** |
| Healthcare workers | Reference | |
| Vaccination statusb) | ||
| Unvaccinated | 2.19 (1.24–3.88) | 0.007** |
| Partially vaccinated | 1.53 (0.76–3.08) | 0.237 |
| Fully vaccinated | Reference |
- 1. World Health Organization (WHO). Pneumonia of unknown cause: China [Internet]. WHO; 2020 [cited 2023 Apr 11]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229.
- 2. World Health Organization (WHO). Novel coronavirus: China [Internet]. WHO; 2020 [cited 2023 Apr 11]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON233.
- 3. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 2020;382:727−33.ArticlePubMedPMC
- 4. Centers for Disease Control and Prevention (CDC). Symptoms of coronavirus disease 2019 (COVID-19) [Internet]. CDC; 2022 [cited 2023 Apr 11]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
- 5. Ki M; Task Force for 2019-nCoV. Epidemiologic characteristics of early cases with 2019 novel coronavirus (2019-nCoV) disease in Korea. Epidemiol Health 2020;42:e2020007.ArticlePubMedPMC
- 6. Yang S, Jang J, Park SY, et al. COVID-19 outbreak report from January 20, 2020 to January 19, 2022 in the Republic of Korea. Public Health Wkly Rep 2022;15:796−805.
- 7. Carter B, Collins JT, Barlow-Pay F, et al. Nosocomial COVID-19 infection: examining the risk of mortality. The COPE-Nosocomial Study (COVID in Older PEople). J Hosp Infect 2020;106:376−84.ArticlePubMedPMC
- 8. Itoh N, Akazawa N, Ishikane M, et al. Lessons learned from an outbreak of COVID-19 in the head and neck surgery ward of a Japanese cancer center during the sixth wave by Omicron. J Infect Chemother 2022;28:1610−5.ArticlePubMedPMC
- 9. Hawkins LP, Pallett SJ, Mazzella A, et al. Transmission dynamics and associated mortality of nosocomial COVID-19 throughout 2021: a retrospective study at a large teaching hospital in London. J Hosp Infect 2023;133:62−9.ArticlePubMedPMC
- 10. Wong SC, Chan VW, Yuen LL, et al. Infection of healthcare workers despite a high vaccination rate during the fifth wave of COVID-19 due to Omicron variant in Hong Kong. Infect Prev Pract 2023;5:100261. ArticlePubMedPMC
- 11. Landoas A, Cazzorla F, Gallouche M, et al. SARS-CoV-2 nosocomial infection acquired in a French university hospital during the 1st wave of the Covid-19 pandemic, a prospective study. Antimicrob Resist Infect Control 2021;10:114. ArticlePubMedPMCPDF
- 12. Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med (Lond) 2020;20:124−7.ArticlePubMedPMC
- 13. Lim J, Jeon S, Shin HY, et al. Case of the index patient who caused tertiary transmission of COVID-19 infection in Korea: the application of lopinavir/ritonavir for the treatment of COVID-19 infected pneumonia monitored by quantitative RT-PCR. J Korean Med Sci 2020;35:e79.PubMedPMC
- 14. McMichael TM, Currie DW, Clark S, et al. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N Engl J Med 2020;382:2005−11.ArticlePubMedPMC
- 15. Chang E, Choi JS, Park TY, et al. A universal screening strategy for SARS-CoV-2 infection in intensive care units: Korean experience in a single hospital. Infect Chemother 2020;52:352−9.ArticlePubMedPMCPDF
- 16. Choi YH. Hospital infection control practice in the COVID-19 era: an experience of university affiliated hospital. Korean J Med 2020;95:308−14.ArticlePDF
- 17. Harada S, Uno S, Ando T, et al. Control of a nosocomial outbreak of COVID-19 in a university hospital. Open Forum Infect Dis 2020;7:ofaa512. ArticlePubMedPMCPDF
- 18. Kim C, Choi G, Park SY, et al. Experience of a COVID-19 outbreak response in a general hospital in Gyeonggi Province, Korea. Epidemiol Health 2021;43:e2021083.ArticlePubMedPMC
- 19. Shang J, Wang J, Adams V, et al. Risk factors for infection in home health care: analysis of national outcome and assessment information set data. Res Nurs Health 2020;43:373−86.ArticlePubMedPMCPDF
- 20. Kim Y. Healthcare policy and healthcare utilization behavior to improve hospital infection control after the Middle East respiratory syndrome outbreak. J Korean Med Assoc 2015;58:598−605.Article
- 21. Park JW, Lee KJ, Lee KH, et al. Hospital outbreaks of Middle East Respiratory Syndrome, Daejeon, South Korea, 2015. Emerg Infect Dis 2017;23:898−905.ArticlePubMedPMC
- 22. Hong NK, Kang KJ. A study on the relationship of infection control performance in a long term care hospital caregivers. J Digit Converg 2020;18:187−98.
- 23. Kim J, Jang E. Factors influencing healthcare-associated infection control of caregivers. J Korean Crit Care Nurs 2021;14:63−75.ArticlePDF
- 24. Choi MJ, Jeong HS, Joung YS, et al. Analysis of needs for infection control education in long-term care hospitals for the epidemic of COVID-19: Borich priority formula and the Locus for Focus model. Health Soc Welf Rev 2021;41:8−21.
- 25. MacLean R, Durepos P, Gibbons C, et al. Education and training for infection prevention and control provided by long-term care homes to family caregivers: a scoping review protocol. JBI Evid Synth 2023;Jan 18 [Epub]. https://doi.org/10.11124/JBIES-22-00308.Article
- 26. Park EJ, Yi S, Kim SJ, et al. Preliminary effectiveness of vaccination for people vaccinated for COVID-19 in the first quarter of 2021. Public Health Wkly Rep 2021;14:1208−11.
- 27. Ahn S, Jang J, Park SY, et al. Outbreak report of COVID-19 during designation of class 1 infectious disease in the Republic of Korea (January 20, 2020 and April 24, 2022). Public Health Wkly Rep 2022;15:1768−72.
- 28. Yi S, Choe YJ, Lim DS, et al. Impact of national Covid-19 vaccination Campaign, South Korea. Vaccine 2022;40:3670−5.ArticlePubMedPMC
References
Figure & Data
References
Citations
 Cite
Cite- Figure
-
- Related articles
-
- Epidemiological characteristics of carbapenemase-producing Enterobacteriaceae outbreaks in the Republic of Korea between 2017 and 2022
- Risk factors for COVID-19 outbreaks in livestock slaughtering and processing facilities in Republic of Korea
- Effectiveness of the COVID-19 vaccine in the Honam region of the Republic of Korea
- Preparedness for the next wave of COVID-19 in the Republic of Korea
- Epidemiological characteristics of varicella outbreaks in the Republic of Korea, 2016–2020
