Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Forthcoming articles > Article
-
Original Article
COVID-19 infection among people with disabilities in 2021 prior to the Omicron-dominant period in the Republic of Korea: a cross-sectional study -
Seul-Ki Kang
 , Bryan Inho Kim
, Bryan Inho Kim -
DOI: https://doi.org/10.24171/j.phrp.2023.0194
Published online: March 28, 2024
Division of Infectious Disease Control, Bureau of Infectious Disease Policy, Korea Disease Control and Prevention Agency, Cheongju, Republic of Korea
- Corresponding author: Bryan Inho Kim Division of Infectious Disease Control, Bureau of Infectious Disease Policy, Korea Disease Control and Prevention Agency, 187 Osongsaengmyeong 2-ro, Osong-eup, Heungdeok-gu, Cheongju 28159, Republic of Korea E-mail: globalepi@korea.kr
© 2024 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 405 Views
- 8 Download
Abstract
-
Objectives
- This study investigated the characteristics of coronavirus disease 2019 (COVID-19) among individuals with disabilities on a nationwide scale in the Republic of Korea, as limited research has examined this population.
-
Methods
- Between January 1 and November 30, 2021, a total of 5,687 confirmed COVID-19 cases among individuals with disabilities were reported through the Korea Disease Control and Prevention Agency’s COVID-19 web reporting system. Follow-up continued until December 24, and demographic, epidemiological, and clinical characteristics were analyzed.
-
Results
- Individuals with disabilities represented approximately 1.5% of confirmed cases, with a mean age of 58.1 years. Most resided in or near metropolitan areas (86.6%) and were male (60.6%). Frequent sources of infection included home (33.4%) and contact with confirmed cases (40.7%). Many individuals (75.9%) had underlying conditions, and 7.7% of cases were severe. People with disabilities showed significantly elevated risk of severe infection (adjusted odds ratio [aOR], 1.63; 95% confidence interval [CI], 1.47–1.81) and mortality (aOR, 1.65; 95% CI, 1.43–1.91). Vaccination against COVID-19 was associated with significantly lower risk of severe infection (aORs for the first, second, and third doses: 0.60 [95% CI, 0.42–0.85], 0.28 [95% CI, 0.22–0.35], and 0.16 [95% CI, 0.05–0.51], respectively) and death (adjusted hazard ratios for the first and second doses: 0.57 [95% CI, 0.35–0.93] and 0.30 [95% CI, 0.23–0.40], respectively).
-
Conclusion
- Individuals with disabilities showed higher risk of severe infection and mortality from COVID-19. Consequently, it is critical to strengthen COVID-19 vaccination initiatives and provide socioeconomic assistance for this vulnerable population.
- A person with a disability, as defined by Article 2 of the Republic of Korea’s Act on Welfare of Persons with Disabilities, is an individual whose daily life or social activities are substantially restricted due to a physical or mental impairment that persists over an extended period. “Physical disability” refers to impairments affecting the body’s primary external functions or internal organs. In contrast, “mental disability” encompasses disabilities resulting from psychological developmental disorders or mental illnesses [1]. In 2020, the number of people with disabilities in the Republic of Korea reached 2,633,026, representing approximately 5.1% of the country’s total population for that year [2].
- According to the “COVID-19 Response Guidelines,” individuals at elevated risk of coronavirus disease 2019 (COVID-19) include older adults aged 65 years or older, residents of long-term care facilities, and those with underlying health conditions [3]. People with disabilities are also considered to be at high risk of COVID-19 infection. Notably, the proportion of people with disabilities who are over 65 years old has been increasing, and these individuals often have permanent disabilities resulting from diseases and accidents, representing a fixed condition [4]. Additionally, the “Infectious Disease Response Manual for Persons with Disabilities” details the vulnerabilities of this group, including “communication restrictions,” “movement restrictions,” “infection vulnerability,” “care in close quarters,” and “group activities.” These factors contribute to the increased risk of COVID-19 infection among people with disabilities [5].
- As such, individuals with disabilities showed higher risk of COVID-19infection; however, additional research is needed. Previous studies examining COVID-19 infection among this population in the Republic of Korea have been constrained by small sample sizes and limited analysis periods. Moreover, studies from an epidemiological perspective are markedly less common than those approached from a social welfare perspective [6,7].
- Therefore, this study was conducted to analyze and present the demographic, epidemiological, and clinical characteristics of confirmed COVID-19 cases among individuals with disabilities from January to November 2021, preceding the Omicron variant.
Introduction
- Materials
- The study period was from the count of confirmed COVID-19 cases as of midnight on January 1, 2021, to the count as of midnight on November 30, 2021. The analysis focused on confirmed COVID-19 cases among individuals with disabilities within this timeframe. During the study period, a total of 386,496 confirmed cases of COVID-19 were reported, with 5,687 of these cases included in our study. Participants were selected according to the following inclusion criteria.
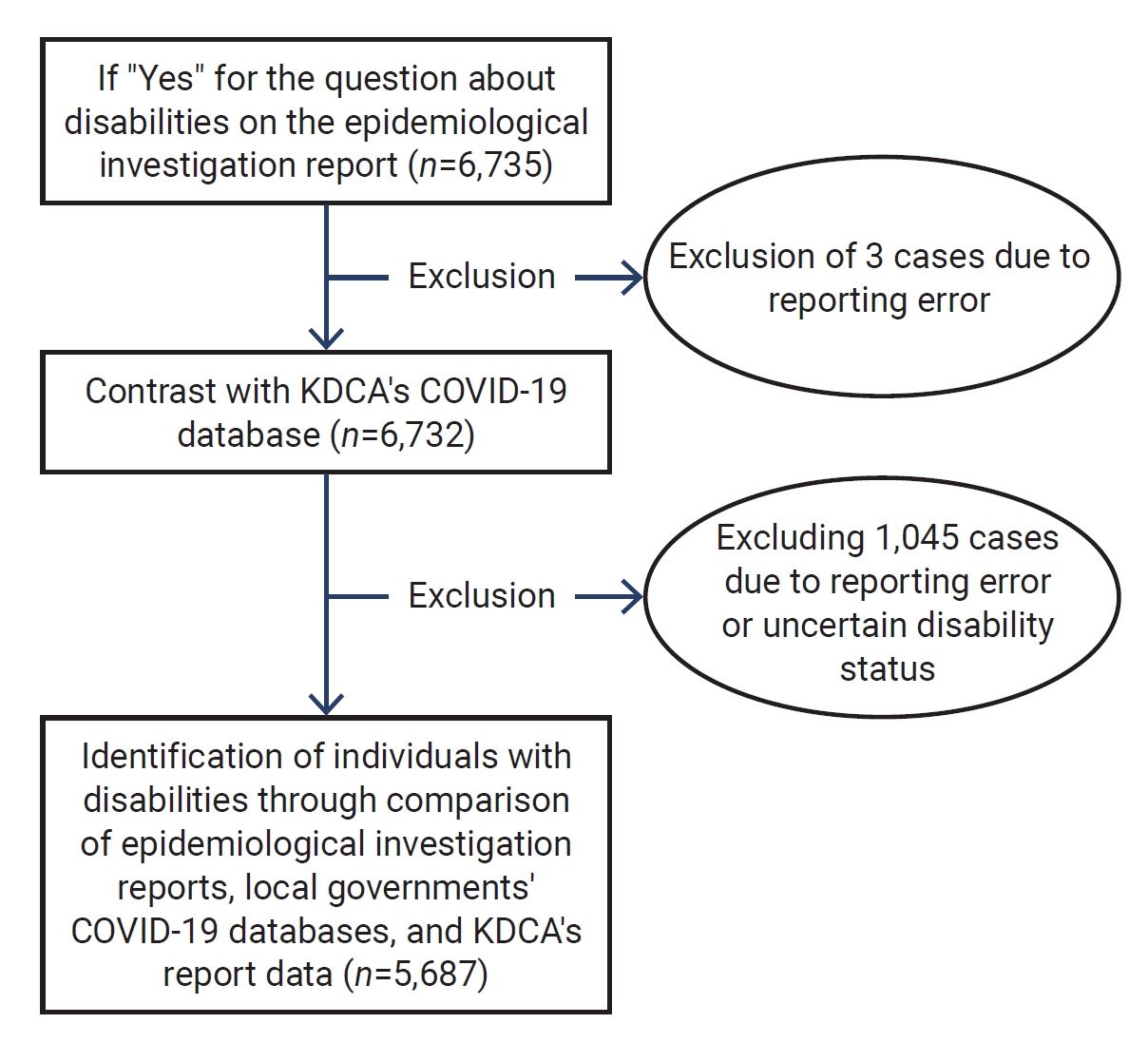
- First, we identified 6,735 confirmed COVID-19 cases among people who indicated that they were registered individuals with disabilities in epidemiological reports of the Korea Disease Control and Prevention Agency (KDCA) on the COVID-19 web reporting system. This list was cross-referenced with the KDCA’s list of confirmed cases, resulting in the exclusion of 3 cases due to delayed reporting registration and errors in the epidemiological report. Subsequently, the list was compared with documentation of confirmed cases managed by each city and provincial government, as well as in-depth epidemiological reports, leading to the exclusion of 1,045 cases due to error or because of unknown information on specific disabilities. Consequently, a total of 5,687 participants were selected for the study. These cases accounted for approximately 1.5% of the cumulative cases during the study period. The analysis of participants was based on the data as of December 24, 2021. The algorithm for the selection procedure of the study participants is shown in Figure 1.
- Epidemiological reports from the COVID-19 web reporting system, along with data regarding confirmed COVID-19 cases provided by the Central Disease Control Headquarters, were used to collect information on demographics, time of infection confirmation, vaccination history, underlying diseases, and routes of epidemiological transmission.
- Methods
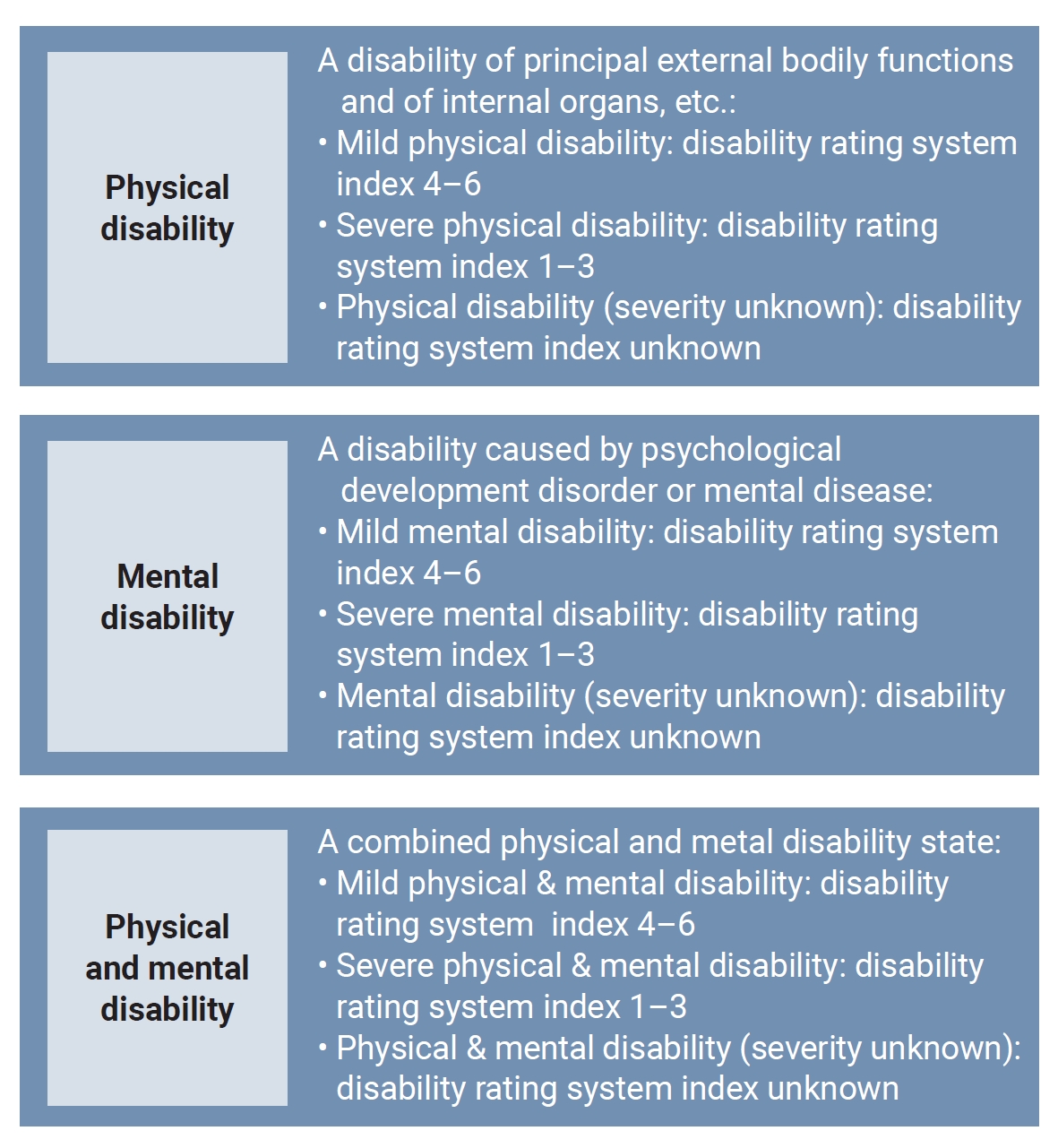
- People with disabilities were categorized based on the presence of physical and/or mental disability, in accordance with the Act on Welfare of Persons with Disabilities [1]. The degree of disability was classified as either non-serious (mild) or serious (severe). This classification was based on the criteria established by the Korea Disabled People’s Development Institute. Mild disability is associated with indices 4 to 6, while severe disability corresponds to indices 1 to 3, according to the disability rating system in use prior to 2019 [8]. The categories of disabilities are detailed in Figure 2.
- The following factors were analyzed: general characteristics, which included demographic information; epidemiological characteristics, which considered the route of transmission and the relationship with previously confirmed cases; vaccination history at the time of COVID-19 diagnosis; underlying conditions; prognosis; comparison with confirmed COVID-19 cases in individuals without disabilities; and clinical characteristics, such as the risk of severe infection, in association with vaccination history and the risk of mortality. Descriptive statistics were used to present the results of the frequency analysis, which were expressed as the corresponding number (n) and percentage (%). Among the clinical characteristics, multivariate logistic regression was used to estimate the adjusted odds ratio (aOR) for the risk of severe infection based on vaccination history. The outcome variable was a binary indicator of severity, and the independent variable was the number of vaccine doses (none, 1, 2, or 3). Adjusted hazard ratios (aHRs) and Kaplan-Meier curves were computed using survival analysis to estimate the risk of mortality. Furthermore, p-values of less than 0.05 were considered statistically significant, and 95% confidence intervals (CIs) were also described. Excel ver. 2013 (Microsoft) and SAS ver. 9.4 (SAS Institute Inc.) were utilized for the statistical analyses.
- Institutional Review Board Approval
- The study protocol received approval from the institutional review board (IRB) of the KDCA, with the approval number IRB-2023-05-08-PE-01.
Materials and Methods
- General Characteristics of Participants
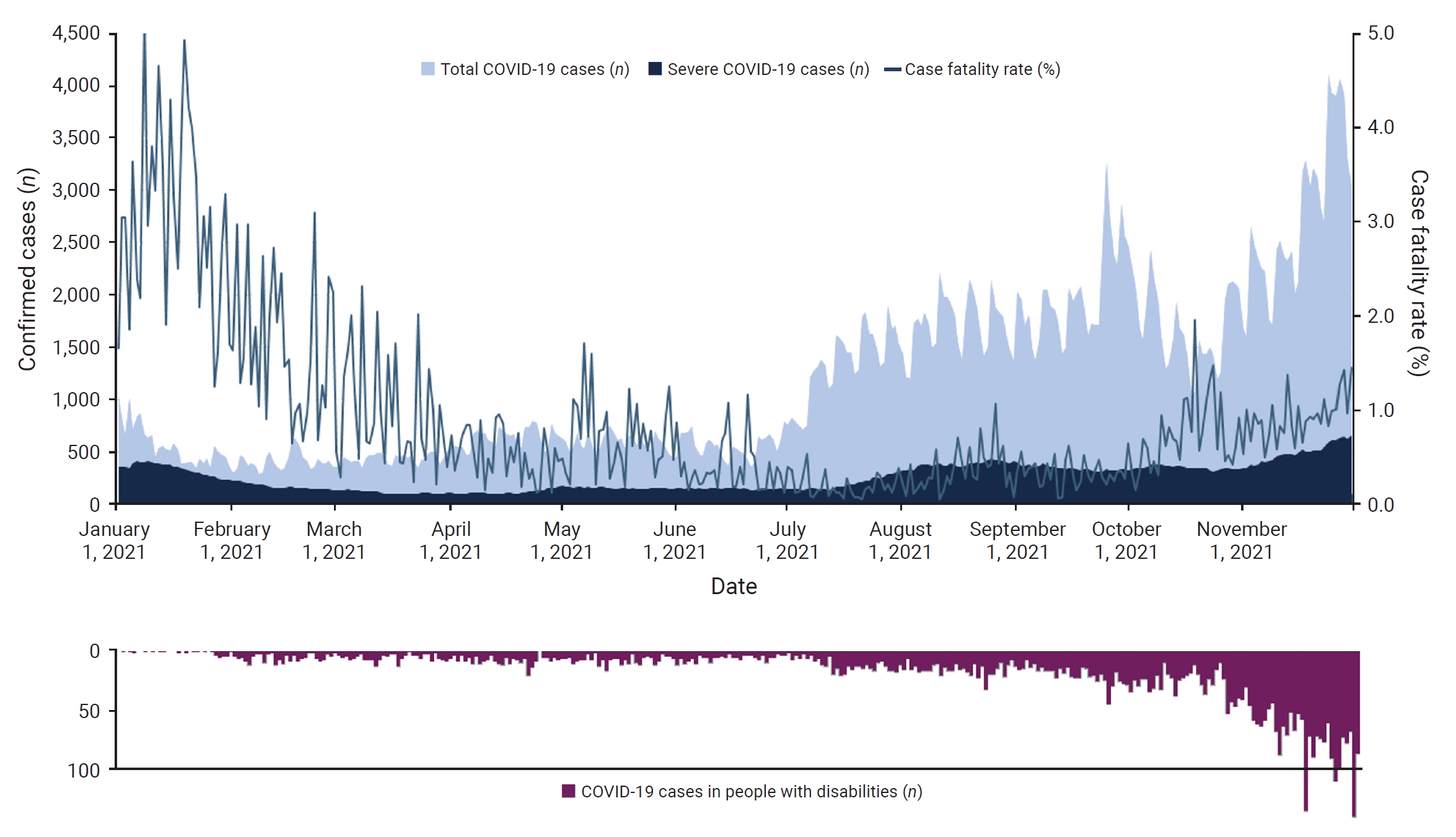
- From January 1 to November 30, 2021, a total of 386,496 cases of COVID-19 were confirmed, with 5,687 of these cases occurring among individuals with disabilities in this study. The temporal trend in the number of confirmed cases is illustrated in Figure 3.
- Substantially more confirmed cases were found among men (n=3,449, 60.6%) than women (n=2,238, 39.4%). The mean age of the patients was 58.1 years, with men averaging 55.9 years and women 61.6 years.
- The categories and degrees of disability are presented in Table 1. Most participants had a physical disability (n=4,310, 75.8%). A total of 1,226 participants had a mental disability (21.6%), and 151 had both physical and mental disabilities (2.7%). Among those with a physical disability, most had a mild physical disability (n=2,637), representing 46.4% of all participants. The distribution of disability categories and degrees was similar between men and women, as shown in Table 1.
- Based on the data from the KDCA COVID-19 web reporting system, most cases resided in urban areas, with 46.6% living in Seoul, 35.5% in Gyeonggi, and 2.9% in Gangwon. According to the Korean Standard Classification of Occupations, nearly half of the participants (n=2,806, 49.3%) were unemployed, while 24.2% were part of the workforce (n=1,378) [9]. The category of “simple labor worker,” which typically refers to low-skilled occupations, was the most frequently reported among both men and women, at 8.3% (n=286) and 4.4% (n=99), respectively.
- Epidemiological Characteristics of Participants
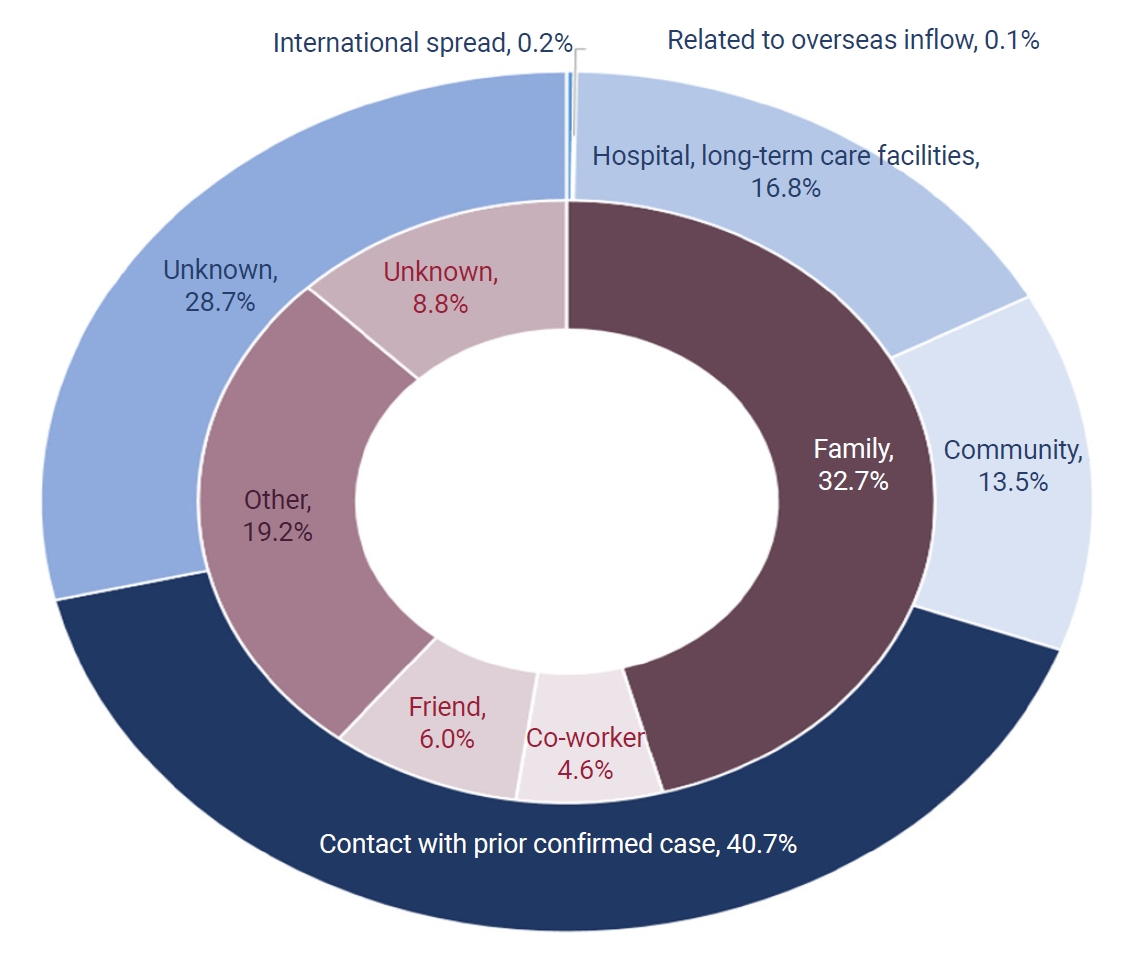
- The location of transmission was domestic—that is, within the Republic of Korea—for 5,674 cases (99.8%). The most common route of transmission was contact with confirmed cases (n=2,316, 40.7%), followed by unknown transmission (n=1,631, 28.7%), outbreaks in hospitals and nursing facilities (n=955, 16.8%), outbreaks in community settings (n=768, 13.5%), and international importation and related transmission (n=17, 0.3%).
- Excluding unknown transmission sources, the most frequent location of exposure was the home (n=1,979, 34.8%), followed by medical facilities (n=552, 9.7%) and nursing facilities (n=323, 5.7%). When analyzed by sex, the most common exposure locations for men were the home (n=1,078, 31.3%), medical facilities (n=312, 9.0%), and the workplace (n=307, 7.0%). For women, the most common exposure locations were the home (n=823, 36.8%), medical facilities (n=240, 10.7%), and nursing facilities (n=212, 9.5%) (Figure 4).
- The most frequent relationship between the participants and previously confirmed cases was either a cohabitating or non-cohabitating family member (n=1,857, 32.7%), followed by another type of contact (n=1,094, 19.2%) and an unknown relationship (n=503, 8.8%).
- Clinical Characteristics of Participants
- An examination of participant prognosis as of December 24, 2021, revealed that 5,073 individuals (89.2%) had been released from quarantine, 378 (6.6%) remained in quarantine, and 236 (4.1%) had died (4.1%). Additionally, 436 participants (7.7%) were classified as severe COVID-19 cases. These patients required either invasive or non-invasive mechanical ventilation, received high-flow oxygen therapy, or underwent extracorporeal membrane oxygenation or continuous renal replacement therapy during the quarantine period due to multiple organ failure.
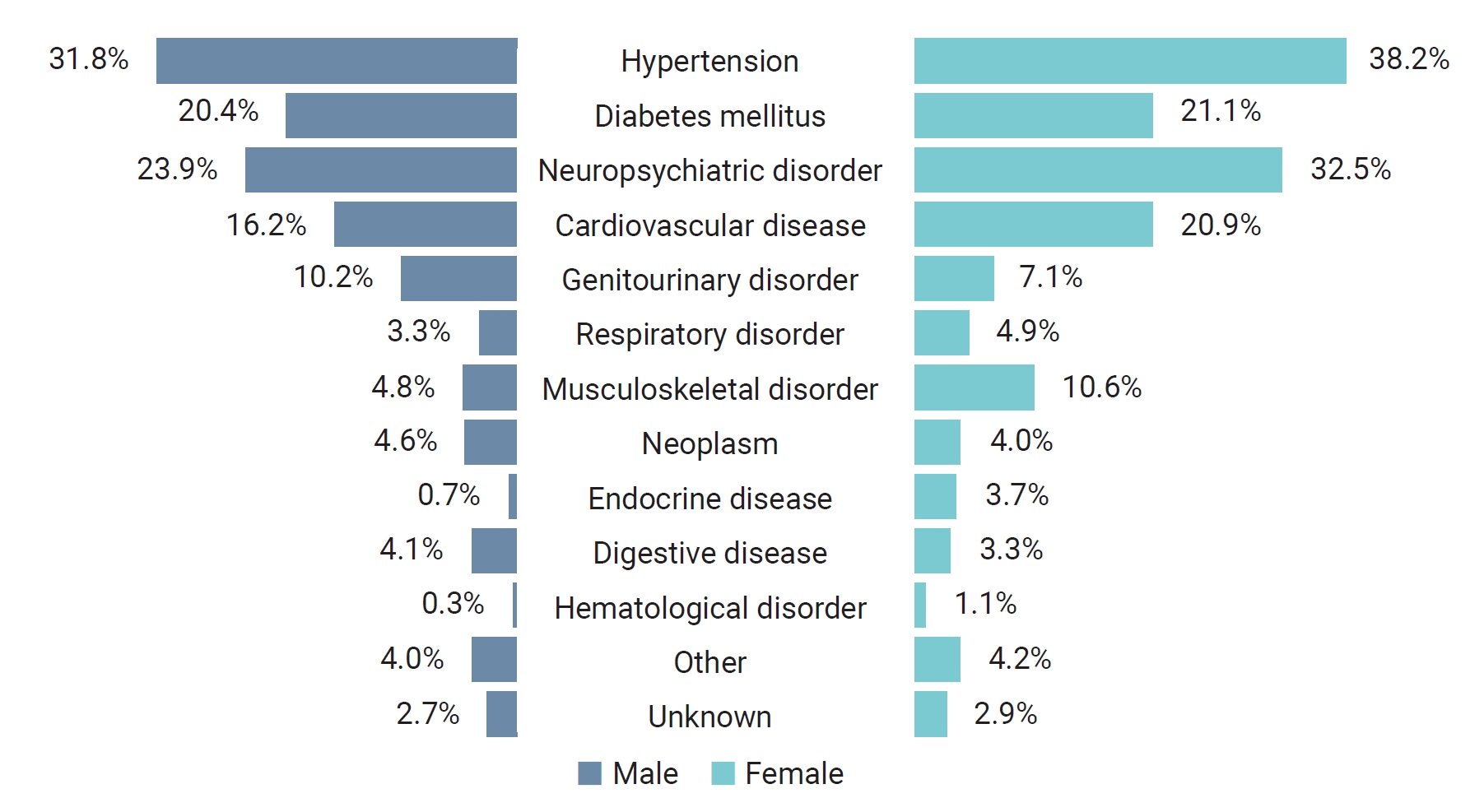
- Among the participants, 4,318 had underlying conditionss, accounting for 75.9% of the total. For both men and women, hypertension was the most common condition, followed by neurological or psychiatric disorders, diabetes, and cardiovascular disease. The fifth most common underlying condition was urologic disease for men and musculoskeletal disease for women, respectively (Figure 5).
- At the time of COVID-19 confirmation, the largest proportion of participants had received 2 vaccination doses (n=2,635, 46.3%). In comparison, 2,388 (42.0%) were unvaccinated, 582 (10.2%) had received 1 dose, and 82 (1.5%) had received 3 doses. When examining the timing of vaccinations, the largest group consisted of unvaccinated individuals (n=2,388, 42.0%). This was followed by 1,307 participants (23.0%) for whom it had been 90 days or more since their second dose, and 649 participants (11.4%) for whom 60 to 90 days had elapsed since their second dose.
- Using multivariate logistic regression analysis, aORs were calculated to identify any significant differences in the risk of severe COVID-19 and mortality between participants and confirmed cases without disabilities across the study period. For this analysis, the number of confirmed cases among people without disabilities was estimated at 380,809, after excluding the participants from the total number of confirmed cases during the study period. The results indicated that the participants were 1.63 times more likely to experience severe COVID-19 infection than people without disabilities (aOR, 1.63; 95% CI, 1.47–1.81). Furthermore, the odds of mortality among participants were 1.65 times higher than among those without disabilities (aOR, 1.65; 95% CI, 1.43–1.91).
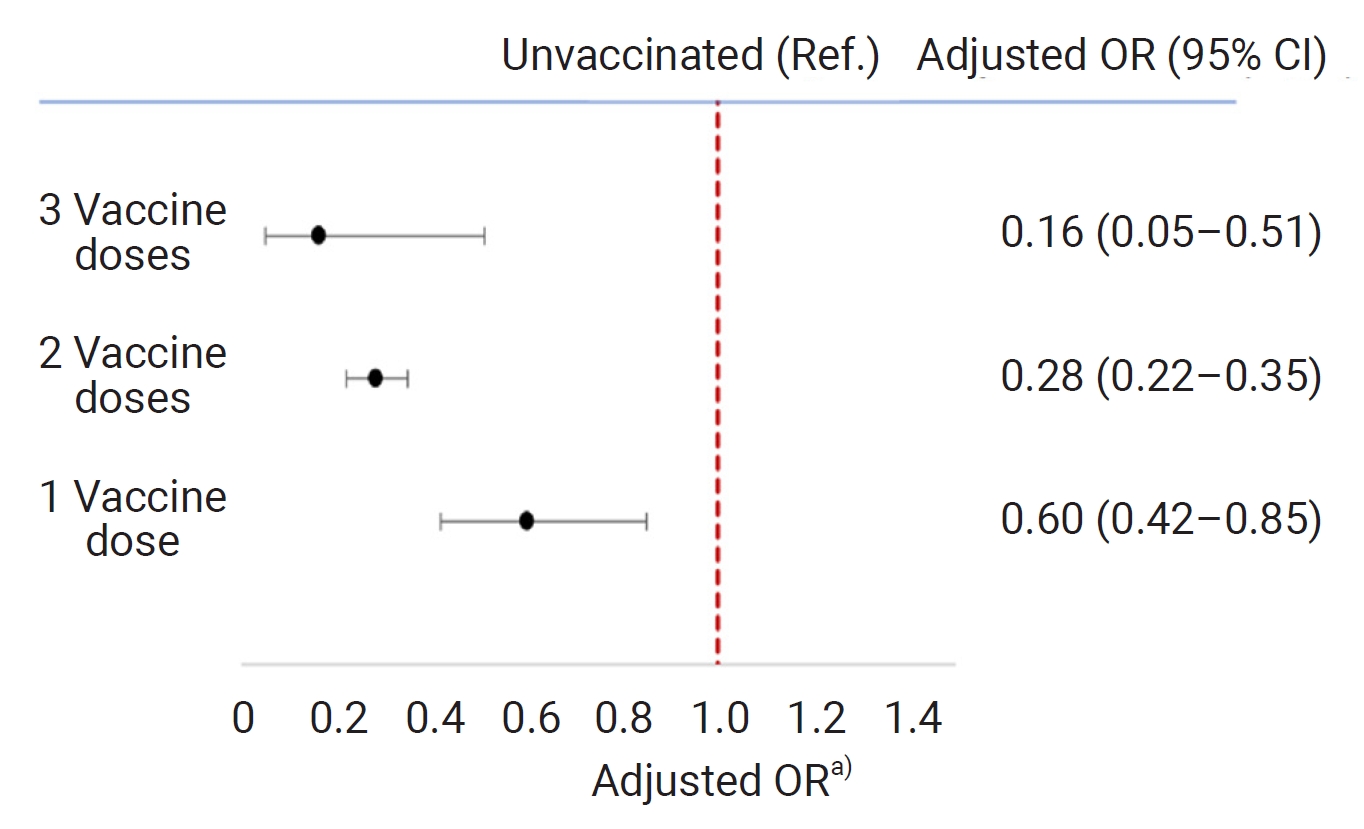
- The risk of severe COVID-19 infection, based on vaccination status at the time of infection confirmation, was analyzed in 4,985 participants (87.7%), excluding those with an unknown degree of disability. The results, adjusted for sex, age, underlying disease, and disability category, are presented in Figure 5. The unvaccinated group served as the reference group. The likelihood of experiencing severe COVID-19 infection was significantly lower in the vaccinated group than in their unvaccinated. Moreover, an inverse relationship was observed between the number of vaccine doses received and the risk of severe COVID-19, indicating that COVID-19 vaccination effectiveness in preventing severe COVID-19 infection(Figure 6).
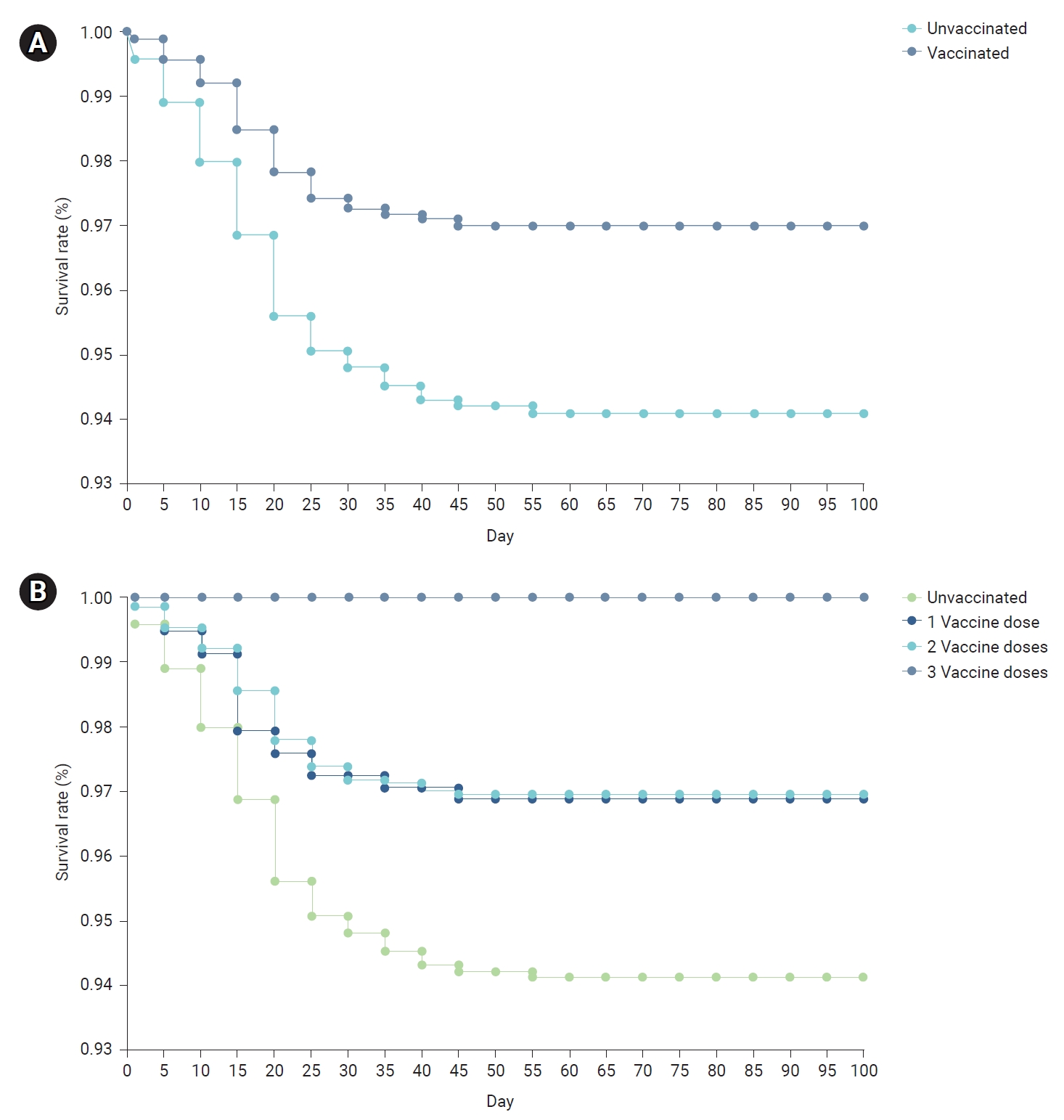
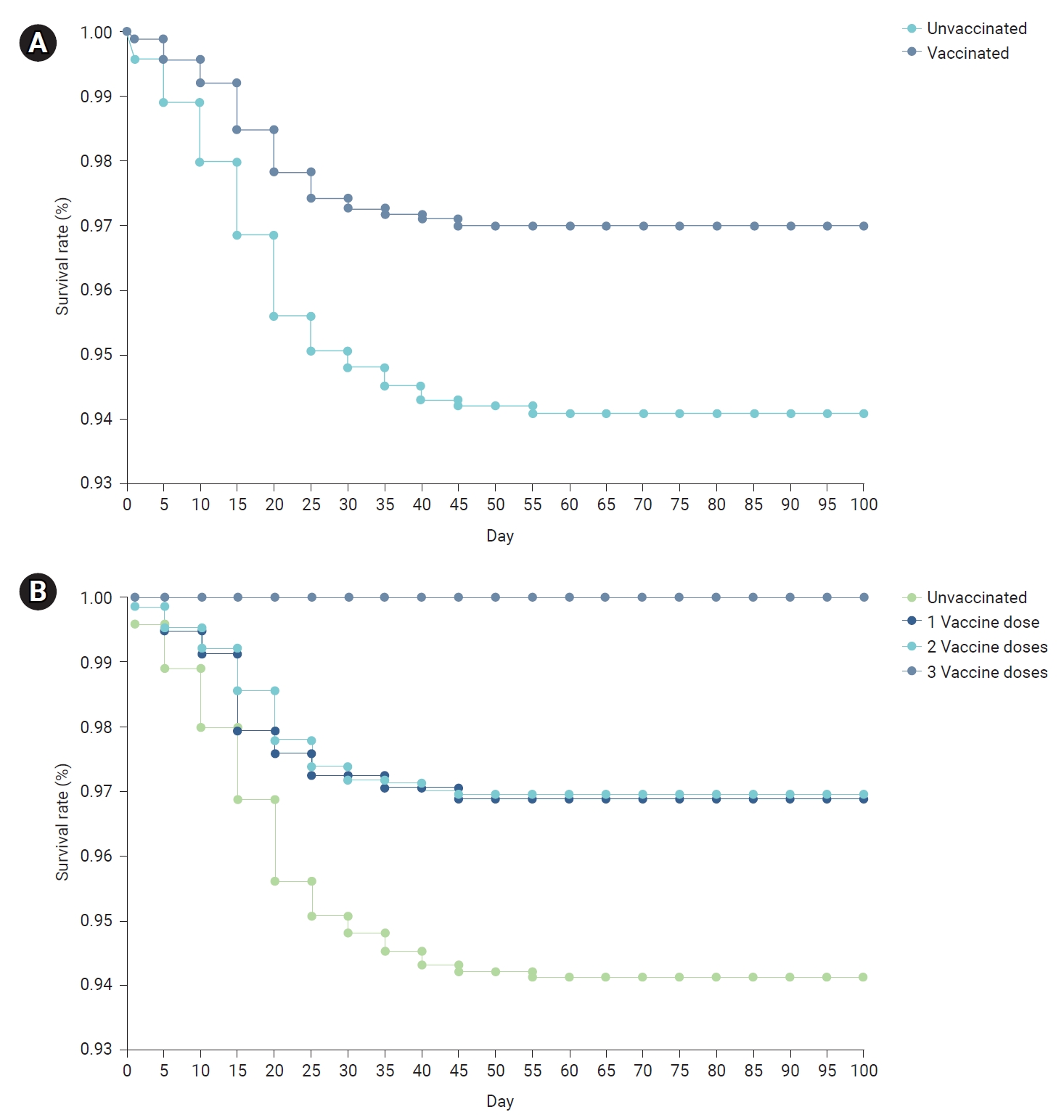
- The time intervals from the date of COVID-19 confirmation to the date of death for deceased participants, and to December 24, 2021, for survivors, were calculated. Survival curves were then constructed and compared using Kaplan-Meier analysis. Significant differences in survival rates were observed based on the history of COVID-19 vaccination and the number of vaccine doses received at the time of COVID-19 confirmation (p<0.001). Specifically, individuals who were vaccinated at the time of COVID-19 confirmation showed a significantly higher survival rate than those who were unvaccinated. Moreover, an increase in the number of COVID-19 vaccine doses at the time of confirmation was associated with a marked increase in the survival rate (Figure 7).
- Table 2 presents the results of an analysis using the Cox proportional hazards model, which was adjusted for variables including sex, age, underlying disease, and disability category. This analysis assessed the risk of mortality associated with overall vaccination status and the number of COVID-19 vaccine doses received at the time of confirmation. The mortality risk among individuals vaccinated against COVID-19 at this time was significantly lower than that of the unvaccinated group (aHR, 0.32; 95% CI, 0.25–0.42). A significantly lower mortality risk was also observed for participants who had received a first vaccine dose (aHR, 0.57; 95% CI, 0.35–0.93) and a second dose (aHR, 0.30; 95% CI, 0.23–0.40). However, among the 82 participants who had received a third vaccine dose, no deaths were reported (Table 2).
Results
Clinical severity and prognosis
Underlying medical conditions and vaccination status at the time ofCOVID-19 confirmation
Comparison of the risk of severe COVID-19 infection and mortality in confirmed COVID-19 cases between individuals with and without disabilities
Analysis of the risk of severe COVID-19 infection and mortality based on COVID-19 vaccination status at confirmation
- In this study, we examined the demographical, epidemiological, and clinical characteristics of 5,687 confirmed COVID-19 cases among individuals with disabilities, from January 1 to November 30, 2021. This timeframe preceded the the Omicron variant dominant period in the Republic of Korea.
- The study participants, all of whom were individuals with disabilities, represented 1.5% of confirmed COVID-19 cases in the Republic of Korea from January to November 2021. The average age of these participants was 58.1 years, with a higher proportion of . By severity, the largest group consisted of those with mild physical disabilities (46.4%), and the majority lived in metropolitan areas. Nearly half of the participants (49.3%) were unemployed, while only 24.2% were economically active, primarily in simple labor work. Consequently, COVID-19 infection is expected to exacerbate not only the health conditions but also the economic conditions of people with disabilities.
- Regarding the location of exposure, the most common route of transmission was infection in the home (33.4%). More generally, the most frequent infection source was contact with individuals already confirmed to have COVID-19 (40.7%), most commonly cohabitating or non-cohabitating family members (32.7%). Therefore, to minimize the incidence of COVID-19 infection among individuals with disabilities, it is essential to encourage self-testing within households and to implement routine testing in medical and nursing facilities. Notably, a previous study indicated that the rate of unknown transmission routes was 20% during the early stages of the COVID-19 pandemic in 2020, whereas in our study, this rate was 28.7% among people with disabilities [10].
- A total of 75.9% of participants had underlying diseases. Regarding prognosis as of December 24, 2021, 4.1% had died, and 7.7% had experienced severe COVID-19 infection. Individuals with disabilities showed significantly higher risk of severe COVID-19 infection and mortality compared to those without disabilities.
- An analysis of vaccination history and the time between COVID-19 vaccination and COVID-19 infection confirmation revealed that the largest group of participants (42.0%) were unvaccinated. This was followed by those for whom 90 days or more had elapsed since the second vaccination dose (23.0%) and those who were 60 to 90 days post-second dose (11.4%). These results indicate that the incidence of COVID-19 increased as the protective effect of the vaccine diminished over time.
- The analysis of COVID-19 risk in relation to the number of vaccine doses revealed a significant reduction in the risk of both severity and mortality. Furthermore, we observed a significant increase in survival rates corresponding with an increase in the number of vaccine doses administered. These findings imply that initial COVID-19 vaccination, along with subsequent doses administered within an appropriate timeframe, have a effectiveness in preventing the COVID-19 severe infectionand mortality in individuals with disabilities.
- This study has a significant value, as it presents a large-scale analysis of the demographical, epidemiological, and clinical characteristics of confirmed COVID-19 cases among individuals with disabilities. The analysis incorporated various perspectives from January 1 to November 30, 2021. However, one limitation of this study is that it may not account for all confirmed COVID-19 cases in this population due to potential data input errors or missing information within the epidemiological investigation data, which served as the primary data source. Additionally, the lack of information on vaccine type precluded an estimation of vaccine effectiveness based on this parameter. Furthermore, while previous research has identified the heterogeneity of infectiousness as a key factor in COVID-19 transmission [11], this study, relying on a national database, lacked the relevant information to consider this factor.
- According to 2021 data from Statistics Korea, 37.7% of all individuals with disabilities are economically active. Among this group, simple labor workers represent the highest proportion, at 28.3%. Furthermore, the percentage of individuals with disabilities aged 65 years or older has been on the rise, increasing from 37.1% in 2010 to 42.3% in 2015 and reaching 48.3% in 2019. Additionally, people with disabilities showed a higher risk of severe COVID-19 and mortality than those without disabilities. Many confirmed COVID-19 cases among people with disabilities involve users of welfare, medical, and nursing facilities. These findings indirectly suggest a high likelihood of chain group transmission if a confirmed case occurs in these facilities. Consequently, people with disabilities are both socially and epidemiologically vulnerable in COVID-19 infection. Therefore, COVID-19 infection is likely to be linked with greater health, economic, and social burden on these individuals.
Discussion
- Considering the decreased number of confirmed COVID-19 cases, the absence of concerning variant viruses, enhanced medical response capabilities, and increased population immunity, the World Health Organization (WHO) declared on May 5, 2023, that COVID-19 was no longer considered a Public Health Emergency of International Concern (PHEIC). This announcement came 3 years and 4 months after the initial PHEIC declaration on January 30, 2020 [12]. Despite this change, the risk of COVID-19 remains, and the WHO has emphasized the implementation of a long-term management system. The Korean government lowered the COVID-19 pandemic national crisis level from the “serious” to the “warning” level on June 1, 2023, reflecting the changed situation [13].
- However, individuals with disabilities still remains as a high-risk group for COVID-19. Therefore, it is crucial to maintain a sustainable means of supporting vulnerable populations, as they are more likely to be affected not only by COVID-19 but also by the next pandemic.
Conclusion
- • Individuals with disabilities faced significantly higher risk of severe coronavirus disease 2019 (COVID-19) infection (adjusted odds ratio [aOR], 1.63; 95% confidence interval [CI], 1.47–1.81) and death (AOR, 1.65; 95% CI, 1.43–1.91) compared to those without disabilities.
- • Vaccination against COVID-19 was associated with significantly reduced risk. The respective AORs for severe infection after 1, 2, and 3 vaccine doses were 0.60, 0.28, and 0.16, with 95% CIs of 0.42–0.85, 0.22–0.35, and 0.05–0.51. For mortality, the adjusted hazard ratios were 0.57 (95% CI, 0.35–0.93) for 1 dose and 0.30 (95% CI, 0.23–0.40) for 2 doses.
HIGHLIGHTS
-
Ethics Approval
The requirement to obtain informed consent was exempted by the Institutional Review Board of the Korea Disease Control and Prevention Agency (2023-05-08-PE-01), as the study included no identifiable information.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Availability of Data
The datasets are not publicly accessible
-
Authors’ Contributions
Conceptualization: all authors; Data curation: SKK; Formal analysis: SKK; Investigation: SKK; Methodology: all authors; Project administration: SKK; Resources: SKK; Supervision: BIK; Visualization: SKK; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Article information

| Variable | Adjusted HR (95% CI)a) | p |
|---|---|---|
| Vaccination | ||
| No | 1 (ref.) | |
| Yes | 0.32 (0.25–0.42) | <0.0001 |
| No. of vaccine doses | ||
| None | 1 (ref.) | |
| 1 | 0.57 (0.35–0.93) | 0.02 |
| 2 | 0.30 (0.23–0.40) | <0.0001 |
| 3 | 0 | 0.96 |
- 1. Act on Welfare of Persons with Disabilities, Act No. 19303 (Sep 29, 2023) [Internet]. Korean Law Information Center; 2023 [cited 2023 May 1]. https://www.law.go.kr/LSW/eng/engLsSc.do?menuId=2&query=Act%20on%20welfare%20of%20persons%20with%20disabilities%20#liBgcolor0.
- 2. Korean Statistical Information Service. Number of the registered disabled-by year, types of disability and gender (the whole country) [internet]. Statistics Korea; 2022 [cited 2023 May 1]. Available from: https://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_11761_N001&vw_cd=MT_ETITLE&list_id=G_22&scrId=&seqNo=&language=en&obj_var_id=&itm_id=&conn_path=A6&path=%252Feng%252Fsearch%252FsearchList.do.
- 3. Korea Disease Control and Prevention Agency (KDCA). Coronavirus disease 2019 response and management guidelines for local governments in South Korea. 10-3th ed. KDCA; 2022. Korean.
- 4. Lee SH, Lee BH. Current status of support for the disabled and policy tasks following the COVID-19 outbreak. Health Welf 2020;22:7−34. Korean.Article
- 5. Ministry of Health and Welfare. Infectious disease response manual for the disabled: focusing on COVID-19. 2nd ed. Ministry of Health and Welfare; 2021. Korean.
- 6. Jeon GB. COVID-19 and the lives of disabled persons: the current status and countermeasures. J Crit Soc Welf 2020;68:173−207. Korean.Article
- 7. Choi JW, Han E, Lee SG, et al. Risk of COVID-19 and major adverse clinical outcomes among people with disabilities in South Korea. Disabil Health J 2021;14:101127. ArticlePubMedPMC
- 8. Korea Disabled People’s Development Institute. Abolition of disability grade system announcement [Internet]. Korea Disabled People’s Development Institute. 2022;[cited 2023 May 1]. Available from: https://www.koddi.or.kr/service/rating_intro.jsp. Korean.
- 9. Statistics Korea. Korean standard classification of occupations. 7th ed. Statistics Korea; 2017. Korean.
- 10. Ryu S, Ali ST, Noh E, et al. Transmission dynamics and control of two epidemic waves of SARS-CoV-2 in South Korea. BMC Infect Dis 2021;21:485. ArticlePubMedPMCPDF
- 11. Lim JS, Noh E, Shim E, et al. Temporal changes in the risk of superspreading events of coronavirus disease 2019. Open Forum Infect Dis 2021;8:ofab350. ArticlePubMedPMCPDF
- 12. World Health Organization. Statement on the fifteenth meeting of the IHR (2005) Emergency Committee on the COVID-19 pandemic [Internet]. World Health Organization; 2023 [cited 2023 May 20]. Available from: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic.
- 13. Korea Disease Control and Prevention Agency (KDCA). Lowering the COVID-19 crisis stage and shifting major quarantine measures [Press release]. KDCA; 2023 [cited 2023 Jun 1]. Available from: https://www.kdca.go.kr/board/board.es?mid=a20501010000&bid=0015&list_no=722664&cg_code=&act=view&nPage=1. Korean.
 Cite
Cite