Sex differences in factors associated with prediabetes in Korean adults
Article information

Abstract
Objectives
Identifying the factors associated with prediabetes is necessary for the early detection and management of high-risk individuals with prediabetes. The purpose of this study was to identify the factors associated with prediabetes according to sex in Korean adults.
Methods
Using the Korean National Health and Nutrition Examination Survey from 2015 to 2019, a total of 13,595 adults (5,565 males and 8,030 females) aged ≥20 years were included in the data analysis. Logistic regression analysis was performed to identify the factors associated with prediabetes according to sex in Korean adults.
Results
In both males and females, age and a family history of type 2 diabetes were associated with prediabetes. In males, current and past smoking habits were associated with increased prediabetes. In addition, low-intensity physical activity and prolonged sedentary behavior were associated with a higher prevalence of prediabetes. Females with a lower education level (less than middle school graduation) showed a higher risk of prediabetes.
Conclusion
Sex-specific prevention strategies for prediabetes should be developed. In addition, older individuals and those with a family history of type 2 diabetes should be screened for prediabetes.
Introduction
Prediabetes is an intermediate metabolic state that is characterized by increased blood glucose levels when compared to normal levels, although not as high as the diagnostic cut-off for diabetes [1,2]. Because individuals with prediabetes do not experience distinctive signs and symptoms, they can be at high risk of developing type 2 diabetes and cardiovascular disease (CVD) [3,4]. According to the National Diabetes Statistics report in 2020, 34.5% of adults over 18 years of age in the United States had prediabetes [5]. In Korea, the prevalence of prediabetes in adults over 30 years was 26.9% in 2018, and the prevalence has continued to increase [6]. Notably, 14.2% to 24.6% of cases of prediabetes in adults over 45 years of age progressed to type 2 diabetes within 10 years [7] and 32.2% of individuals with a diagnosis of type 2 diabetes had CVD approximately 10 years after being diagnosed [8]. Thus, the long-term healthcare burden of unmanaged prediabetes causes substantial public health problems. In this context, we emphasize the need for early identification of at-risk individuals and the early management of prediabetes before the development of type 2 diabetes [9,10]. Identification of the factors associated with prediabetes is required for early intervention and detection of high-risk individuals with prediabetes [11]. Sociodemographic factors (e.g., age, sex, and education level), cardiometabolic factors (e.g., dyslipidemia and hypertension), and behavioral factors (e.g., smoking habits and physical activity) associated with prediabetes have been identified in previous studies [11−14]. However, the reported risk factors for prediabetes have been inconsistent among studies [14,15]. Differences in ethnicity and sex might have contributed to these disparities among studies, in addition to differing definitions of prediabetes [11,16].
In previous studies, the prevalence of prediabetes and the factors associated with prediabetes differed according to ethnicity [10,17]. Furthermore, in individual ethnic groups, factors associated with prediabetes varied according to sex [10,11,16]. According to a systematic review by Siddiqui et al. [14], smoking and alcohol consumption were significantly associated with prediabetes in males, while poor dietary habits were strongly associated with prediabetes in females. That study emphasized the identification of sex differences in factors associated with prediabetes, which would be helpful for developing sex-specific prevention strategies for those at risk of type 2 diabetes [14].
According to a conceptual model that explains the development of risk factors and health status related to CVD [18], risk factors and health status (e.g., obesity, type 2 diabetes, and dyslipidemia) related to CVD were associated with sociodemographic determinants (e.g., age, sex, education level, household socioeconomic status), internal health resources/burdens (e.g., psychosocial discomfort), external health resources/burdens (e.g., social support and familial status), and health behaviors (e.g., diet, smoking habit, physical activity). Based on a literature review, this study categorized the factors associated with prediabetes into sociodemographic factors (age, sex, education level, and household socioeconomic status), internal health resources/burdens (stress and depression), external health resources/burdens (living with a spouse, and a family history of type 2 diabetes), and health behaviors (habit of eating out, current and past smoking, current alcohol consumption, physical activity, and sedentary behavior). Adjustments were also made for CVD risk factors (covariates) that are significantly associated with prediabetes, including adiposity (obesity), abdominal obesity, hypertension, high triglyceride (TG) levels, low levels of high-density lipoprotein cholesterol (HDL-C), and high total cholesterol levels.
This study aimed to identify the associations of sociodemographic, internal health resources/burdens, external health resources/burdens, and health behavioral factors with prediabetes after controlling for covariates according to sex in Korean adults.
Materials and Methods
Study Design and Population
A cross-sectional study design was applied with a secondary analysis of the Korean National Health and Nutrition Examination Survey (KNHANES) from 2015 to 2019. A total of 39,759 adults aged ≥20 years (18,181 males and 21,578 females) participated in the KNHANES. Among them, 26,170 adults who had prediabetes (11,838 individuals) and normal blood glucose levels (15,332 individuals) were primarily selected after excluding 13,589 adults, including pregnant females and individuals who were diagnosed and treated for stroke, angina, myocardial infarction, and diabetes. Finally, 13,595 adults (5,565 males, 8,030 females) aged ≥20 years were included in the data analysis after excluding 13,575 individuals who had incomplete questionnaires, physical examinations (e.g., weight, height), and laboratory tests (e.g., fasting plasma glucose [FPG] and hemoglobin A1c [HbA1c]) that provided the measurements for the variables used in this study (Figure 1).
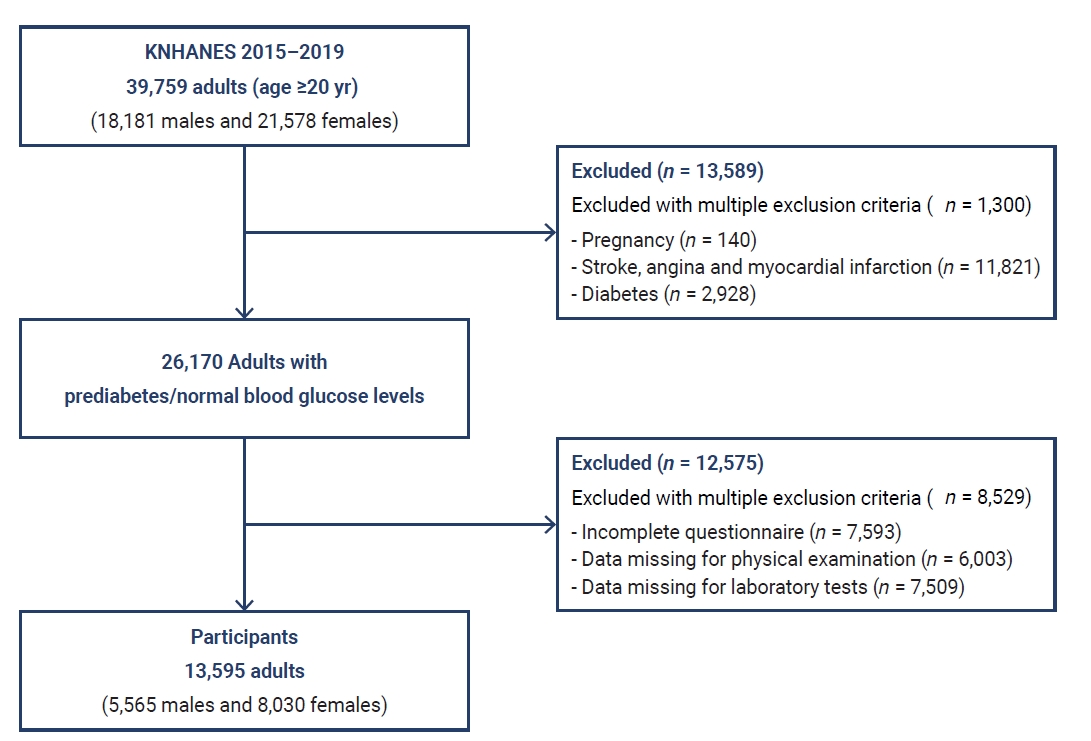
Sampling process. KNHANES, Korean National Health and Nutrition Examination Survey.
Measurements
Dependent variable
Independent variables
Sociodemographic factors
Age was categorized into 20s to 30s, 40s to 50s, and ≥60s. Sex was categorized as male or female. Education level was categorized as less than middle school graduation, high school graduation, or college graduation. Household socioeconomic status was categorized as low, middle, and high.
Internal health resources/burdens
Daily stress was determined with a single question, with response categories of “severe,” “a little,” and “not at all.” To evaluate depression, respondents were asked if they had been diagnosed with depression by a psychiatrist, with a response of yes or no.
External health resources/burdens
Marital status was categorized as living with a spouse or living without a spouse (separated, divorced, bereaved, and unmarried). The family history of type 2 diabetes was categorized as yes or no.
Health behaviors
To evaluate the habit of eating out, the average frequency of eating out in the previous year was determined with a single question, and the response was categorized as “more than once a day” or “less than once a day.” Smoking habits were categorized as current, past, or never, and current alcohol consumption was categorized as “yes” or “no.” For the intensity of physical activity (work, travel to and from places, and leisure), metabolic equivalent task (MET)‐minutes were calculated from activities in a week [20]; >600 MET‐minutes a week was considered moderate to vigorous intensity and <600 MET‐minutes a week was considered low intensity. To evaluate sedentary behavior, the number of hours spent sitting or lying down in a day was determined with a single question, and sedentary hours a day were categorized as <8 hours a day or ≥8 hours a day, with the latter being considered prolonged sedentary behavior [21].
Covariates
To evaluate adiposity, body mass index (BMI) was calculated using height and weight. Based on BMI, participants were categorized as non-obese or obese. The non-obese category included underweight (<18.5 kg/m2) and normal weight (≥18.5 kg/m2 and <23 kg/m2), and the obese category included overweight (≥23 kg/m2 and <25 kg/m2) and obesity (>25 kg/m2) [22]. Abdominal obesity was assessed by waist circumference: a waist circumference >90 cm in males and >85 cm in females indicated abdominal obesity [22]. Hypertension was regarded as a blood pressure >130/85 mmHg and/or use of antihypertensive therapy. Other covariates included high total cholesterol, high TG (TG >150 mg/dL and/or treatment for hypertriglyceridemia), and low HDL-C (HDL-C <50 mg/dL and/or therapy for low HDL-C).
Statistical Analysis
Complex sampling analysis was performed with IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA) following the data analysis guidelines recommended by the KNHANES. The characteristics of prediabetes, sociodemographic factors, internal and external health resources/burdens, health behavior, and covariates were analyzed using frequencies and percentages. As the first step in logistic regression analysis, univariate logistic regression was conducted to identify the association between each independent and outcome variable. Controlling for covariates, multivariate logistic regression analysis was then performed to identify the factors associated with prediabetes according to sex in Korean adults.
IRB/IACUC Approval
This study was approved by the Institutional Review Board of Chungnam National University and was exempted from review because it was a secondary analysis (202111-SB-242-01).
Results
The prevalence of prediabetes was 40.9% in males and 34.4% in females (Table 1). The sociodemographic, internal health resources/burdens, external health resources/burdens, and health behavioral characteristics of the males and females are presented in Table 1.

Characteristics of prediabetes: sociodemographic factors, internal health resources/burdens, external health resources/burdens, and health behaviors according to the participants’ sex
The factors associated with prediabetes in males are presented in Table 2. In the univariate logistic model for prediabetes in males, age and education level were the sociodemographic factors associated with the prevalence of prediabetes. The following age groups were associated with a lower likelihood of developing prediabetes in males: 20s to 30s (crude odds ratio [COR], 0.17; 95% confidence interval [CI], 0.15–0.19; p<0.001) and 40s to 50s (COR, 0.61; 95% CI, 0.54–0.68; p<0.001). The following factors were associated with a higher risk of developing prediabetes in males: (1) lower education level (less than middle school graduation) (COR, 1.26; 95% CI, 1.14–1.40; p<0.001); (2) among internal health resources/burdens, severe stress (COR, 1.28; 95% CI, 1.14–1.47; p<0.001) or “a little” stress (COR, 1.22; 95% CI, 1.10–1.37; p<0.001); (3) among external resources/burdens, a positive family history of type 2 diabetes (COR, 1.38; 95% CI, 1.27–1.51; p<0.001); and (4) among health behaviors, eating out more than once a day (COR, 1.28; 95% CI, 1.16–1.39; p<0.001), current smoking (COR, 1.98; 95% CI, 1.78–2.19; p<0.001), previous smoking (COR, 2.63; 95% CI, 2.38–2.90; p<0.001), low-intensity physical activity (COR, 1.49; 95% CI, 1.32–1.67; p<0.001), and prolonged sedentary behavior for ≥8 hours a day (COR, 1.39; 95% CI, 1.28–1.52; p<0.001).

Factors associated with prediabetes in males
In the multivariate logistic model for prediabetes in males, age was associated with the prevalence of prediabetes. Participants in their 20s to 30s (adjusted odds ratio [AOR], 0.28; 95% CI, 0.22–0.36; p<0.001) and 40s to 50s (AOR, 0.64; 95% CI, 0.51–0.79; p<0.001) had a lower likelihood of developing prediabetes. Among external health resources/burdens, a family history of type 2 diabetes was also associated with a higher likelihood of developing prediabetes (AOR, 1.17; 95% CI, 1.01–1.35, p=0.037). Among health behaviors, current smoking (AOR, 1.35; 95% CI, 1.13–1.63, p=0.001) and past smoking (AOR, 1.29; 95% CI, 1.09–1.53, p=0.004) were associated with a higher likelihood of developing prediabetes. Low-intensity physical activity (AOR, 1.37; 95% CI, 1.19–1.59; p<0.001) and prolonged sedentary behavior for ≥8 hours a day (AOR, 1.22; 95% CI, 1.06–1.41, p=0.006) were associated with a higher likelihood of developing prediabetes in males. The logistic regression model was found to fit the study variables (F=33.29, p<0.001).
The factors associated with prediabetes in females are presented in Table 3. In the univariate logistic model for prediabetes in females, the sociodemographic factors of age and education level were associated with the prevalence of prediabetes. Younger age groups were associated with a lower likelihood of developing prediabetes: 20s to 30s (COR, 0.09; 95% CI, 0.08–0.10; p<0.001) and 40s to 50s (COR, 0.34; 95% CI, 0.31–0.37; p<0.001). The following factors were associated with a higher likelihood of developing prediabetes in females: (1) lower education level (less than middle school graduation) (COR, 2.91; 95% CI, 2.64–3.20; p<0.001); (2) among internal health resources/burdens, severe stress (COR, 1.89; 95% CI, 1.67–2.13; p<0.001), “a little” stress (COR, 1.61; 95% CI, 1.45–1.79; p<0.001), and depression (COR, 1.46; 95% CI, 1.24–1.72; p<0.001); (3) among external health resources/burdens, a family history of type 2 diabetes (COR, 1.41; 95% CI, 1.31–1.53; p<0.001); and (4) among health behaviors, eating out more than once a day (COR, 1.92; 95% CI, 1.72–2.17; p<0.001), a history of smoking (COR, 1.52; 95% CI, 1.27–1.82; p<0.001), current alcohol consumption (COR, 1.61; 95% CI, 1.47–1.75; p<0.001), low-intensity physical activity (COR, 1.27; 95% CI, 1.14–1.39; p<0.001), and prolonged sedentary behavior for ≥8 hours a day (COR, 1.36; 95% CI, 1.26–1.46; p<0.001).

Factors associated with prediabetes according in females
In the multivariate logistic model for prediabetes in females, lower education level (less than middle school graduation) showed an association with a higher likelihood of developing prediabetes (AOR, 1.21; 95% CI, 1.04–1.41, p=0.014). The logistic regression model was found to fit the study variables (F=46.28, p<0.001).
Discussion
This study identified the factors associated with prediabetes according to sex in Korean adults and showed that the prevalence of prediabetes was higher in Korean males than in Korean females. Previous studies also reported a higher prevalence of prediabetes in males [16,23,24]. Sex differences in the prevalence of impaired fasting glucose were associated with biological, psychosocial, and health behavior factors [25]. In previous studies, in addition to the common non-modifiable biological risk factors (e.g., age, family history), males had more lifestyle-related risk factors such as smoking and binge alcohol drinking than females [16,26].
Similarly, the current study showed that a current or past smoking habit, low-intensity physical activity, and prolonged sedentary behaviors are associated with a higher risk of prediabetes in Korean males only. In previous epidemiological studies, smoking was also associated with the development of type 2 diabetes [27,28]. The nicotine in cigarettes binds to nicotinic acetylcholine receptors in neuronal and non-neuronal or visceral organs, and these receptors participate in signaling within metabolic tissues (e.g., pancreatic islets, adipose tissue) [29]. Thus, nicotine exposure might lead to a proinflammatory metabolic state that could affect insulin sensitivity and beta-cell function [29]. In addition, Zoli and Picciotto [30] suggested that smoking might be associated with adverse fat distribution, including abdominal obesity, which contributes to worse glucose intolerance and insulin sensitivity. According to a cohort study of Korean adults [31], smoking was significantly associated with an increased probability of treatment for type 2 diabetes in both males and females. The risk increased in a dose-dependent manner as the amount of cumulative smoking increased [31]. Furthermore, the cumulative dose-dependent influence of smoking on the development of type 2 diabetes continued after smoking cessation, although smoking cessation had a beneficial effect on reducing the risk of type 2 diabetes [32]. Because the smoking prevalence in Korea is higher in males and females, a current and past smoking history might be more significantly associated with the development of prediabetes in males and females. Similarly, in a previous study of Koreans in their 20s–30s, current smoking was associated with prediabetes in males only. In this context, smoking prevention and smoking cessation should be emphasized as a means of preventing prediabetes in adults, especially for males who have a higher prevalence of smoking.
Physical activity showed an inverse association with insulin resistance as a fundamental contributor to impaired fasting glucose in individuals with or without prediabetes [33]. According to a systematic review, physical activity was effective in improving oral glucose tolerance in individuals with prediabetes [34]. In addition, a meta-analysis of randomized trial studies showed that physical activity had a beneficial effect on reducing fasting blood glucose and HbA1c levels in healthy individuals as well as individuals with prediabetes and type 2 diabetes [35]. Robles-Ordaz et al. [24] reported the preventive effects of physical activity on prediabetes in males and females aged >20 years. However, the beneficial effects of physical activity on insulin sensitivity were dose-dependent, with a combination of intensity, duration, and frequency [36]. Bird and Hawley [37] reported that moderate-intensity physical activity of ≥30 minutes per day for 3 to 5 days a week was associated with improved insulin sensitivity and glycemic control. Moreover, they suggested that repeated regular physical activity produced beneficial long-term effects on insulin sensitivity [37]. Males are more likely to participate in physical activities such as exercise, leisure, and social activities than females. In Korea, this may be associated with the traditional Confucian Korean culture, which recommends differing types of activity for males and females. From an early age, Korean males mainly participate in dynamic physical activities, while females are more involved in static sedentary behaviors. Thus, the association between activity levels and prediabetes might be more significant for males than for females. In a 10-year longitudinal study of Chinese adults who have similar cultural backgrounds, increased physical activity was effective in resolving prediabetes and restoring normal glucose levels in males only [38]. Regular moderate and vigorous physical activity should be encouraged to prevent prediabetes among adults.
According to a systematic review [39], increased sitting time may also result in the increased occurrence of type 2 diabetes. Hamilton et al. [40] reported that the contractile activity of skeletal muscle has a critical influence on the development of type 2 diabetes. Similarly, objective sedentary time and insulin sensitivity were inversely associated [41]. Sedentary behaviors include sitting and reclining positions such as during TV watching and might be associated with eating more snacks during a time when metabolic activities are at resting levels [42,43]. Thus, prolonged sedentary behavior during waking time can result in increased adiposity (BMI) from increased calorie intake and reduced energy metabolism. According to Kautzky-Willer et al. [44], increasing adiposity resulted in reduced insulin sensitivity in both males and females, although females tended to have better insulin sensitivity than males. They also proposed that sex hormones (estrogen) might demonstrate antidiabetic effects [44]. Therefore, even when increased adiposity is associated with prolonged sedentary behavior, males might show a worse decrease in insulin sensitivity than females. In this context, sedentary behaviors should be reduced to prevent prediabetes among adults with increased insulin resistance. Replacing 30 minutes of sitting time with low-intensity activity improved insulin sensitivity by 5% in individuals with a greater risk of type 2 diabetes [45]. Physical activity, even low-intensity physical activity, should replace sedentary behavior to help prevent prediabetes. Based on the results of this study, males tended to have more risky health behaviors associated with prediabetes. To develop sex-specific intervention strategies for the prevention of prediabetes, healthcare providers need to be aware of the development of prediabetes in males and be able to detect the risky health behaviors associated with prediabetes.
Individuals with high education levels have greater access to health-related resources that provide information and assistance in following a healthy lifestyle [46]. Despite the association of lower education levels to increased glucose intolerance in males, the effect of educational inequality (lower education levels in females) on glucose intolerance in females was much more significant in a previous study [46]. Furthermore, educational inequality among individuals with glucose intolerances such as type 2 diabetes was more prominent in Korean and Chinese females than Korean and Chinese males, regardless of socioeconomic status [47,48]. Traditionally, Korean society has regarded males as being superior to females, and education was prioritized accordingly, although this males superiority was a stronger influence decades ago. Therefore, elderly Korean females had lower education levels compared to males of the same age. Accordingly, in a previous study of adults aged >45 years from China, a culture similar to Korea’s, data showed that educational inequality was more prevalent in females than in males [46]. Data also revealed that females with low education levels tended not to follow the behavioral guidelines for obesity prevention [46] and showed maladaptive reactions to health information for the prevention of CVDs, ultimately rejecting the health promotion behaviors meant to prevent CVDs [49]. To encourage and promote healthy behaviors among individuals with low education levels, sufficient support should be provided to help these individuals successfully incorporate the health information into their lifestyles.
Age and a family history of type 2 diabetes have often been associated with prediabetes and type 2 diabetes [25,50], and age is a strong determinant of type 2 diabetes [25]. In one study, the prevalence of type 2 diabetes increased with age up to approximately 65 years, with no significant change in prevalence in later ages [51]. Similarly, according to a previous study conducted in adults aged 35 to 64 years in China and Sweden, the prevalence of prediabetes gradually increased with age in males and females [25]. In addition, in a previous meta-analysis, individuals with a family history of type 2 diabetes showed a 1.4-fold increased risk of prediabetes [50]. Thus, Wagner et al. [50] proposed that a family history of type 2 diabetes might be linked to hepatic insulin resistance, and Katulanda et al. [52] proposed that a family history might reflect genetic vulnerability as a meaningful predictor and assessment tool for prediabetes and type 2 diabetes. Finally, older individuals and those with a family history of type 2 diabetes should be routinely screened for prediabetes as a primary risk group for prediabetes.
Using national data, this study identified sex differences in the factors associated with prediabetes in Korean adults. However, this study had several limitations. First, because we used a cross-sectional design, a causal association between prediabetes and the potentially associated factors was not confirmed. Therefore, longitudinal cohort studies are required. Second, although the age of the participants ranged from the 20s to 60s, this study did not identify the factors associated with prediabetes according to age. Thus, future studies should report age differences among the factors associated with prediabetes. Third, in previous studies, ethnic differences were found in the factors associated with prediabetes. Thus, further studies should focus on comparing the factors associated with prediabetes according to race or ethnicity.
Conclusion
The results of this study showed a higher rate of prediabetes in Korean males than in Korean females. Age and a family history of type 2 diabetes were associated with prediabetes in both males and females. However, regarding health behaviors, current and past smoking habits, low-intensity physical activity, and prolonged sedentary behavior were significant factors in male but not in females. Thus, sex-specific prevention strategies for prediabetes should be developed, and older individuals and those with a family history of type 2 diabetes should be screened for the risk of prediabetes.
Notes
Ethics Approval
This study was approved by the Institutional Review Board of Chungnam National University (202111-SB-242-01), was exempted from review because it was a secondary analysis (202111-SB-242-01), and was performed in accordance with the principles of the Declaration of Helsinki.
Conflicts of Interest
The author has no conflicts of interest to declare.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (Ministry of Science and ICT) (2021R1A2C100682811).
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.