Epidemiological characteristics of carbapenem-resistant Enterobacteriaceae and carbapenem-resistant Acinetobacter baumannii in a tertiary referral hospital in Korea
Article information

Abstract
Objectives
This study aimed to identify the epidemiological characteristics of patients with carbapenem-resistant Enterobacteriaceae and Acinetobacter baumannii (CRE/CRAB) isolates in a tertiary referral hospital in Korea.
Methods
We collected and analyzed data from 528 adults admitted to a tertiary referral hospital from August 1, 2018 to February 29, 2020. The CRE/CRAB isolates were confirmed as being present at the time of patients’ admission or acquired during hospitalization based on their medical records. The t-test, chi-square test, or Fisher exact test and stepwise multiple logistic regression were performed.
Results
While the proportion of community-acquired CRE/CRAB was low (6%), 20% of CRE/CRAB isolates were identified in patients at the time of hospitalization. The risk of CRAB isolation was positively associated with mechanical ventilator use (odds ratio [OR], 3.52; 95% confidence interval [CI], 1.96−6.33) and total parenteral nutrition use (OR, 3.64; 95% CI, 1.87−7.08).
Conclusion
Over 20% of CRE/CRAB isolates in a tertiary referral hospital in Korea were found at the time of patients’ admission. Furthermore, patients with mechanical ventilation and/or total parenteral nutrition tended to acquire CRAB more frequently. Thus, active surveillance for CRE/CRAB at the time of hospitalization is strongly required, particularly for patients who are expected to require mechanical ventilation or total parenteral nutrition.
Introduction
The World Health Organization declared antibiotic resistance to be 1 of 10 international health threats to human life, and pointed out problems such as the prolongation of hospital stays, the economic burden due to the use of expensive antibiotics, death, and disability [1]. For some carbapenem-resistant organisms (CROs), genes encoding carbapenemases are located in mobile genetic elements, such as plasmids or transposons; these can cause rapid transmission of resistant bacteria between patients [2,3], making them highly likely to spread from healthcare settings to the local community [4]. In Korea, carbapenem-resistant Enterobacteriaceae (CRE) and multidrug-resistant Acinetobacter baumannii are designated as infectious diseases that must be reported to health authorities by law [5]. According to the United States Centers for Disease Control and Prevention (CDC), CRE and carbapenem-resistant Acinetobacter baumannii (CRAB) are classified as the most urgent threats among antibiotic-resistant microorganisms, for which reason the CDC has strengthened antibiotic resistance management [6].
Several studies have investigated the epidemiological characteristics and risk factors of acquiring CROs in patients admitted to intensive care units (ICUs) and organ transplantation wards in the United States [7], those admitted to a general hospital for CRE [8]; those admitted to the Taiwan General Hospital for CRAB [9], those admitted to an acute care health hospital for carbapenem-resistant Gram-negative bacteremia in Taiwan [10]; and CRE-infected patients in acute care health hospitals in China [11]. Those studies also sought to describe the prevalence, incidence, and epidemiological characteristics of multidrug-resistant Gram-negative bacteria and CROs, including colonization and infection in ICUs, using data entered into a German infection monitoring system [12]. However, relatively few studies have been conducted in Korea; examples include a study aiming to identify risk factors for CRE colonization in patients admitted to the ICUs of general hospitals [13,14] and a study on the acquisition of carbapenem-resistant Escherichia coli in hospitalized patients [15]. These studies mainly targeted patients admitted to the ICU and focused on CRE. Therefore, limited information is available on the epidemiological characteristics of CROs in other hospital settings, including general wards, and other types of CROs, such as CRAB. In addition, a case of CRE acquisition in a patient who had not visited a hospital within 3 months was reported [16], and approximately 30% of cases confirmed at hospitals are found within 48 hours of hospitalization [17]. Therefore, it is necessary to understand the characteristics of CRE/CRAB isolates, including both healthcare-acquired (HA) and community-acquired (CA) CRE/CRAB, but few studies on CA CRE/CRAB have been reported in Korea. The purpose of this study was to identify the epidemiological characteristics of patients from whom CRE/CRAB was isolated among those admitted to a tertiary referral hospital, and to conduct a comparison between CRE and CRAB isolates, and between CA and HA CRE/CRAB.
Materials and Methods
Study Design and Participants
This was a retrospective cohort study that used patients’ medical records. It was conducted at Inje University Busan Baik Hospital, an 800-bed tertiary referral hospital in Busan, Republic of Korea. The participants were CRE/CRAB cases who met all the following criteria: (1) adult patients aged 19 years or older, (2) admitted to any ward, including the emergency room and ICU, from August 1, 2018 to February 29, 2020, and (3) confirmed to have CRE/CRAB either by a CRE active surveillance culture using a rectal swab or on a culture using blood or another clinical specimen. Both colonization and infection were included. In this hospital, active CRE surveillance culture is conducted only for patients admitted to the ICU, and all departments collect clinical samples when necessary for culture and antibiotic resistance tests. During the study period, only the initial hospitalization and isolate were included in cases of rehospitalization and duplicate isolations of CRE or CRAB, and only the initial isolate was included if both CRE and CRAB were isolated. In total, 65,337 patients were hospitalized during the study period, and CRE/CRAB isolation was confirmed in 528 patients (isolation rate, 0.81%).
Definition and Variables
Cases were defined following the recommendations of the Korea Disease Control and Prevention Agency based on the recommendations of the Clinical and Laboratory Standards Institute (M100-S27) [18,19]. Antimicrobial susceptibility to carbapenems was assessed using the disk diffusion method. CRE was defined based on resistance to imipenem (≤19 mm), meropenem (≤19 mm), or ertapenem (≤18 mm), and CRAB was defined based on resistance to imipenem (≤18 mm) or meropenem (≤14 mm). The CA group was defined as having confirmed CRE/CRAB at the time of hospitalization or within 48 hours of hospitalization, and the HA group was defined as patients transferred from a long-term care facility, regardless of the period, or in whom isolates were obtained after 48 hours of hospitalization in an acute care hospital. The variables examined in this study were general characteristics, multidrug-resistant organism (MDRO)-related characteristics, treatment-related characteristics, and clinical outcomes, referring to the questions used in previous studies [7,11,13] on the characteristics of CRE or CRO isolation. General characteristics included sex, age, hospitalization route, history of hospitalization within 6 months, comorbidities, and the Charlson comorbidity index score (CCIS). MDRO-related characteristics included whether the MDRO was isolated before CRE/CRAB acquisition, the CRE/CRAB acquisition time, specimen source, and strain. Treatment-related characteristics included invasive procedures performed during hospitalization and invasive devices and drugs used for more than 48 hours. Status at discharge was analyzed as a clinical outcome.
Data Collection
With the help of the infection control office of the study hospital, one researcher obtained a list of patients with confirmed CRE/CRAB isolates and selected those who met the inclusion criteria. Data were collected using structured data sheets from electronic medical records, including nursing care, hospitalization-related information, prescriptions, operations, procedures, and diagnostic test results. The CCIS was calculated directly by the researcher, referring to each patient's medical record. When a history of admission to medical institutions other than the study hospital or MDRO isolation was not confirmed, we classified these variables as “unknown.” Treatment-related characteristics prior to admission to the study hospital could not be collected due to a lack of information in the medical record. For every CA or HA case transferred from a long-term care facility, data collection was based on the time of hospitalization. For HA cases with CRE/CRAB confirmed after hospitalization, the data collection period was from the time of hospitalization to the date of CRE/CRAB isolation.
Data Analysis
The collected data were analyzed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). The 2-tailed test was performed at a significance level (α) of 0.05. Frequency and percentage, mean and standard deviation, and median and interquartile ranges were calculated for the characteristics of the study participants. The t-test, chi-square test, or Fisher exact test was performed to compare characteristics between the CRE and CRAB groups and the CA and HA groups. With significant variables from the bivariate analysis as explanatory variables, we calculated the odds ratio and its 95% confidence interval using stepwise multiple logistic regression analysis after confirming the absence of deviation from the assumption of multi-collinearity using a coefficient of determination of less than 0.80 [20].
IRB/IACUC Approval
Prior to data analysis, this study was approved by the Institutional Review Board of Inje University Busan Baik Hospital (20-0114), and the requirement for written consent was waived.
Results
Characteristics of Study Participants
Among the 528 study participants, CRAB was isolated in 67.6%, and 94.1% of cases were HA. At the time of hospitalization, 20.8% of the participants had either CRE or CRAB (Table 1). Tables 2-4 show the characteristics of the study participants. Overall, 63.4% were males, their mean age was 67.7 years, 72.2% had a history of hospitalization within the last 6 months, 49.2% had been transferred from other healthcare facilities, and 50.0% had a history of diagnosed hypertension. Regarding MDRO history, 22.0% had vancomycin-resistant Enterococcus, followed by extended-spectrum β-lactamase–producing organisms (16.7%). The majority of CRE/CRAB isolates occurred in respiratory specimens (60.0%), and the major strains were A. baumannii (67.6%) and Klebsiella spp. (23.9%). Almost one-third (32.6%) of participants died before discharge. During hospitalization, 51.4% underwent surgery, 90.9% used a urinary catheter, 84.2% used a central venous catheter, and 54.5% used carbapenem as an antimicrobial agent.

Distribution of CRE and CRAB isolates (n=528)

Comparison of general characteristics, MDRO-related characteristics, and clinical outcome between patients with CRE and those with CRAB

Factors associated with CRAB isolation (n=418)
Comparison of Characteristics between the CRE and CRAB Group, and the CA and HA Group
There were significant differences in the characteristics of the CRE and CRAB groups with regard to the history of hospitalization within 6 months, hypertension, treatment in the ICU, MDRO history, the source of the specimen from which CRE/CRAB was isolated, and the use of arterial catheters, mechanical ventilation, and total parenteral nutrition (TPN) (Tables 2 and 3). Compared to the CRE group, the CRAB group showed lower frequencies of hospitalization within 6 months (p=0.006), hypertension (p=0.007), VRE history (p=0.019), and broad-spectrum β-lactamase–producing organism history (p<0.001), but higher frequencies of ICU stay (p=0.001), arterial catheter use (p=0.001), mechanical ventilator use (p<0.001), and TPN use (p<0.001). CRE was more prevalent in rectal swab specimens at the time of hospitalization, whereas CRAB was more prevalent in respiratory specimens after hospitalization (both p<0.001) (Tables 2 and 3). Multiple logistic regression analysis showed that CRAB isolation was positively associated with mechanical ventilator use and TPN use. The risk of CRAB isolation was 3.52 times higher in those who used a mechanical ventilator and 3.64 times higher in those who used TPN compared to their counterparts (Table 4).

Comparison of treatment-related characteristics between patients with CRE and those with CRAB
The CA and HA groups showed significant differences in hospitalization route, hypertension, cerebrovascular disease, treatment in the ICU, MDRO history, and the source of the specimen from which CRE/CRAB was isolated (Table 5). The HA group showed higher frequencies of transfer from other healthcare facilities (p<0.001), cerebrovascular disease (p=0.011), and treatment in the ICU (p<0.001), and lower frequencies of hypertension (p=0.016), MDRO history (p<0.001), and extended-spectrum β-lactamase-producing organism history (p=0.004) compared to the CA group (Table 5). Multiple logistic regression analysis showed that the risk of HA-CRE/CRAB isolation was 6.30 times higher in patients diagnosed with cardiovascular disease than in those without cardiovascular disease (Table 6).
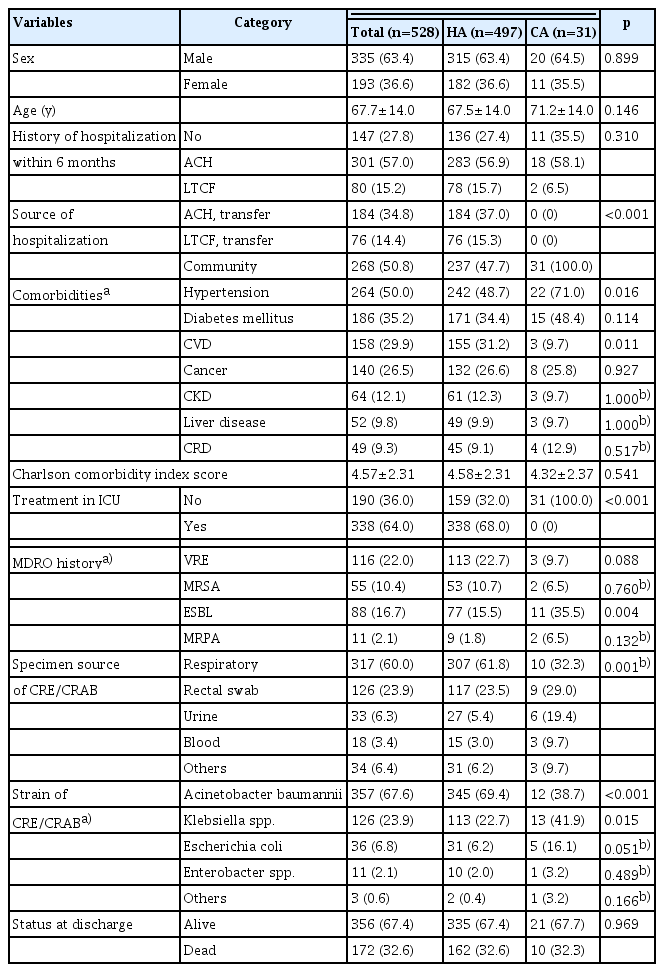
Comparison of general characteristics between patients with healthcare-acquired and community-acquired infections

Factors associated with healthcare-acquired CRE and CRAB isolation (n=528)
Discussion
In this study, we identified the epidemiological characteristics of patients with confirmed CRE or CRAB isolation among inpatients in wards and the ICU, and compared the characteristics between the CRE and CRAB groups and between the HA and CA groups.
CRAB isolation was common in this tertiary hospital in Korea, suggesting that A. baumannii constitutes a large proportion of carbapenem-resistant bacteria in domestic medical institutions. According to the results of the global antimicrobial resistance surveillance system in Korea (Kor-GLASS) from 2016 to 2019, the imipenem resistance rates were 0.1% in blood and 0.1% in urine for E. coli, 1.0% in blood and 1.2% in urine for Klebsiella pneumoniae, and 90.3% in blood for A. baumannii, which was a very alarming finding [21]. The reported types of CROs differ across studies. CROs isolated from carbapenem-resistant bloodstream infections in Taiwan were higher in Acinetobacter spp. and Pseudomonas spp. than in CREs, including E. coli, Klebsiella spp., and Enterobacter spp. [10]. In contrast, a study on carbapenem-resistant Gram-negative bacteremia at a university hospital in the United States [22] and a study in the ICU and transplant ward of a university hospital in the United States [7] showed the order of Pseudomonas aeruginosa and K. pneumoniae, indicating that the isolation rate of Actinetobacter spp. was lower than that of other strains.
A. baumannii is commonly found in hospital environments and is known to cause various healthcare-associated infections, such as sepsis, pneumonia, urinary tract infections, wound infections, and postoperative infections [23]. Most strains are resistant to various antibiotics, including carbapenem [24,25]. In the Kor-GLASS analysis, the majority of Enterobacteriaceae cases were community-associated, whereas 86.9% of Actinetobacter spp. Cases were healthcare-associated [21]. Although A. baumannii is a Gram-negative bacterium, it tolerates a dry environment well [26]. Many CRAB epidemics have been reported in healthcare settings, including ICUs, and the vulnerability to these outbreaks has been increasing due to the growing number of patients with underlying diseases, invasive catheters, and mechanical ventilation, as well as the use of broad-spectrum antibiotics [27–29]. In this study, 64% of participants received ICU treatment, and many participants underwent invasive procedures and received antibiotic treatment, which may explain the higher rate of CRAB isolation.
The risk of CRAB isolation increased with mechanical ventilator use and TPN use. TPN use was also confirmed as a risk factor for CRAB bloodstream infection in a of patients at the Taiwan Veterans Hospital [9]. In this study, TPN was used by approximately 88% of the participants. Therefore, we can expect that MDRO prevention and control measures, including thorough hand hygiene, will lead to significant reductions in MDROs, including CRAB, among TPN-using patients [18,30].
Approximately 6% of the participants in this study were found to have CA infections. The percentage of CA infections relative to HA infections varied from 6% [31] to 10% [8] in the United States and from 12% [32] to 30% [17] in Taiwan. According to the results of this study, it would be difficult to say that CRE/CRAB is prevalent in communities in Korea; however, continuous monitoring is required considering the possibility of its spread to the community. CRE and CRAB are designated as legally notifiable infectious diseases and are under mandatory and sentinel surveillance systems, respectively [5,33]. Therefore, it is possible to determine whether spread has occurred to the local community by reporting HA and CA separately to health authorities. Although there were relatively few CA infections in this study, 1 out of 5 CRE/CRAB was isolated at the time of hospitalization among CRE/CRAB isolated patients, suggesting that CRE/CRAB management at the time of hospitalization is important.
Similar to previous studies [7], the primary hospitalization route of patients was from the community, followed by transfer from acute care hospitals and transfer from long-term care facilities. Approximately half of the participants were transferred from acute care hospitals and long-term care facilities. Approximately 70% of the study participants had a history of hospitalization within 6 months, and about 65% to 90% of patients had a history of hospitalization within 1 year in a previous study in the United States [8]. Thus, for patients with a history of hospitalization within 6 months to 1 year, a system for active surveillance cultures is required at the time of hospitalization. However, for hospitals to which a large number of patients are transferred, such as the hospital in this study, the application of active surveillance culture for all inpatients and outpatients would be burdensome in terms of time and cost. As an alternative, selectively performing active monitoring cultures for high-risk groups by applying a previously developed risk model can be considered [8,13,14].
Most patients had invasive devices within 3 months of the survey, with urinary catheters being the most prevalent, followed by central venous catheters, gastrointestinal tubes, arterial catheters, and mechanical ventilators. According to previous studies, although the duration of keeping invasive devices varied from 30 days to 3 months from the point of the survey, the most common type of invasive device was the urinary catheter [7,9,10,13]. Among drugs other than antibiotics, gastric acid inhibitors (including proton pump inhibitors or histamine H2 receptor antagonists) were frequently used among the patients in this study, consistent with a previous study [7].
The mortality rate at discharge in this study was 32.6%, which was higher than the 17.0% reported in a previous domestic study [13] on the isolation of CRE from patients admitted to the ICU, with a 30-day mortality rate of 14.2% to 24.8% [22], in patients whose culture was positive for carbapenem-resistant Gram-negative bacteremia during hospitalization between 2000 and 2017 at a hospital in the United States. Patients with CRAB have been reported to have a lower survival rate than those with other carbapenem-resistant Gram-negative bacteremia [22]. Considering the previous study [22], the relatively high mortality rate in this study may be related to the higher proportion of CRAB compared to CRE.
Strengths and Limitations
This study is significant in that it identified and analyzed the characteristics of all hospitalized patients in whom CRE or CRAB was isolated, including those in the emergency department and the ICU. However, this study has the following limitations that need to be considered when interpreting its results. First, the number of CRE/CRAB cases may have been underestimated because active surveillance cultures were only performed for patients admitted to the ICU, and only the first case was included in the analysis when both CRE and CRAB were isolated. Second, this study was limited to CRE and CRAB among carbapenem-resistant Gram-negative bacteremia, according to the MDRO management policy of the research institution. Third, for cases of HA infections in patients who were transferred from long-term care facilities or acute care hospitals, the length of stay and treatment-related characteristics at the previous institutions could not be considered due to data limitations. Fourth, the data on patients’ general characteristics were based on the “history taking” results in patients’ electronic medical records, as collected at the time of hospitalization. Therefore, the responses for certain items, such as history of hospitalization within 6 months and comorbidities, may have been biased. Finally, this study cannot be generalized to other types of medical institutions because the data were collected from a tertiary referral hospital.
Conclusion
Over 20% of CRE/CRAB isolates in a tertiary referral hospital in Korea were found at the time of admission. Furthermore, CRAB isolation occurred more frequently in patients with mechanical ventilation and/or TPN than in those without. Thus, active surveillance of CRE/CRAB at the time of hospitalization is strongly required, particularly for patients who are expected to require mechanical ventilation or TPN.
Notes
Ethics Approval
This study was approved by the Institutional Review Board of Inje University Busan Baik Hospital (20-0114), and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was waived.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
The datasets are not publicly available but are available from the corresponding author upon reasonable request.