
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 3(1); 2012 > Article
-
Articles
Application of the Microagglutination Test for Serologic Diagnosis of Human Brucellosis - Sang-Hee Park, Yoo-Hoon Lee, Hyuk Chu, Seon-Do Hwang, Kyu-Jam Hwang, Hee-Yeol Choi, Mi-Yeoun Park
-
Osong Public Health and Research Perspectives 2011;3(1):19-23.
DOI: https://doi.org/10.1016/j.phrp.2012.01.003
Published online: December 31, 2011
Division of Zoonoses, Korea National Institute of Health, Osong, Korea.
- Corresponding author. E-mail: miyeoun@korea.kr
• Received: October 28, 2011 • Revised: December 15, 2011 • Accepted: January 5, 2012
Copyright ©2012, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License () which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- Brucellosis is one of the most common zoonoses in the world, and occurs mainly in farmers, slaughterhouse workers, and veterinarians via direct or indirect contact with infected animals or their products. The clinical symptoms of human brucellosis are nonspecific, such as fever, headache, chills, and sweating. Diagnosis and treatment of brucellosis requires laboratory tests. Although the serum tube agglutination test (SAT) is the standardized gold method, it is laborious, time consuming, and requires a number of reagents. A microagglutination test (MAT) variant of the SAT or enzyme-linked immunosorbent assay (ELISA) is recommended for serological diagnoses. For the simple and rapid diagnosis of brucellosis, the MAT was standardized using samples for the SAT to define positive and negative categories, and we then compared the sensitivity and specificity of the MAT and ELISA.
-
Methods
- Thirty SAT-positive sera and 60 SAT-negative sera were used in this study. Antibody titers of ≥1:160 were considered positive readings in both the SAT and MAT. Brucella abortus antigens and Brucella-positive control antiserum were used in the SAT and MAT. ELISAs of IgM and IgG were performed according to the manufacturers’ instructions.
-
Results
- The titers of the MAT differed according to antigen concentration. The optimal concentration of B abortus antigen was determined to compare the sensitivity and specificity between the MAT and SAT. The sensitivity and specificity of the MAT were 93.3% and 96.7%, respectively, for IgG with reference to ELISA, and 96.7% and 98.3%, respectively, for IgM.
-
Conclusions
- The optimal concentration of antigen for the MAT was 1:10. The MAT is less time consuming and requires less antigen and serum than the SAT. The results of the MAT showed good agreement with those of ELISA. The results of this study suggest that the MAT could be useful for diagnosis of brucellosis.
- Brucellosis, caused by species of the Gram-negative bacterium Brucella, continues to be a problem in humans and animals throughout the world [1]. In Korea, brucellosis is an endemic disease, and B abortus is the prevailing strain in human infections [2]. Human brucellosis occurs among livestock workers and veterinarians who live and work in rural areas with cattle farms [3].
- Clinically, Brucellosis is highly polymorphic and induces inconstant fever, sweating, weakness, anemia, headache, and depression [4]. Since the symptoms are similar to those associated with other febrile diseases, laboratory tests are required for the diagnosis and treatment of brucellosis [5]. Although confirmation of brucellosis requires isolation of the bacteria from blood, several serological tests have been developed to facilitate the diagnosis of human brucellosis: the serum tube agglutination test (SAT), anti-human globulin test, indirect fluorescence antibody assay (IFA), and enzymelinked immunosorbent assay (ELISA) [6]. The most frequently used method for diagnosing human brucellosis is serological screening with the SAT. Although the SAT is a frequently performed method, it is laborious, time consuming, and requires a number of reagents, so it is unsuitable as a primary test in laboratories with a large specimen workload. The SAT is not convenient for field use or for conducting serologic surveys in the support of epidemiologic investigations. Several rapid screening tests have been proposed, but variations in antigens, incubation times, and interpretations of significant reactivity make it difficult to evaluate their suitability for screening human sera. The microagglutination test (MAT) has the advantage of being able to process a large number of samples. ELISA may differentiate between IgG and IgM antibodies. These have shorter run times and require less training than agglutination tests in interpreting results [2,7].
- The purpose of this study was to standardize the MAT for the simple and rapid diagnosis of brucellosis using samples for the SAT to define positive and negative categories. In addition, the utility of the SAT, MAT, and ELISA as diagnostic tools for human brucellosis were evaluated.
1. Introduction
- 2.1. Sera and antigen
- Thirty serum samples from 30 patients with acute brucellosis and 60 from healthy individuals were included in this study. All serum samples were referred between 2005 and 2009 for further laboratory diagnosis under the suspicion of brucellosis. Appropriate Brucella positive and negative sera (BD, Spark, Maryland, USA) were used for all agglutination tests, as well as for controls. The diagnosis of brucellosis was based on clinical findings along with identification of Brucella or the presence of serum antibodies (SAT titer ≥1:160). The antigen used was a commercial suspension of B abortus (Germaine, San Antonio, Texas, USA and BD, Spark, Maryland, USA), prepared according to the manufacturers’ instructions. Titrations were made by serial two-fold dilutions with 0.85% saline.
- 2.2. Serum tube agglutination test (SAT)
- For the SAT, the procedural methods described previously [8] were used. The working dilution of antigen for the SAT was a 1:50 dilution of Brucella suspension in 0.85% saline. Doubling dilutions of serum were made with saline in tubes, from 1:10 to 1:1280 dilution. High, low, and negative reference sera of known titers were used as controls. Each tube contained 0.5 ml of diluted serum, to which an equal amount of the 1:50 dilution (working dilution) of the antigens was added. The contents of the tubes were mixed, and the tubes incubated in a 37℃ shaking incubator for 24 h.
- 2.3. Microagglutination test
- The MAT was performed with a commercial Brucella antigen as described previously [9], in 96-well U-shaped microplates. Serial two-fold dilutions of the sera were made in saline from 1:10 and to 1:1280. The MAT was performed by incubating the sera at 37℃ for 24 h.
- Each of the 90 sera were tested against Brucella using tube agglutination as well as by microagglutination. Appropriate positive and negative serum controls were used for all tests as well as for controls. Before examination of the unknown sera by the agglutination test, each antigen was tested to determine the optimal concentration of the antigen dilution necessary for the highest agglutination titer with specific antisera in the MAT. To determine the optimal concentration, serial two-fold dilutions of the antigens were tested against similar dilutions of each control serum in a “block” or “checkerboard” titration (Figure 1). Dilutions of sera from 1:5 to 1:640 were made directly in microtiter plates.
- 2.4. Enzyme linked immunosorbent assay (ELISA)
- ELISA of IgG and IgM were performed and interpreted using a commercial kit (Panbio, Brisbane, Queensland, Australia) according to the manufacturer’s instruction. Serum was diluted 1:100 in the diluents provided with the ELISA kit before transfer to Brucella antigen-coated microcells strips for 20 min at room temperature (100 mμ/well). Bound IgM was detected after a washing with phosphate-buffered saline containing 0.05% Tween 20, a 20-min incubation with antihuman IgM peroxidase (100 μl/well), another washing, and a 10-min incubation with tetramethylbenzidine
- substrate (100 μl/well). The reaction was stopped by the addition of 100 μl of 1 M phosphoric acid per well, and the strips were read at 450 nm. Each run included positive, negative, and cutoff calibrator controls. An index value (Panbio units) was calculated to generate the results for either IgG or IgM as follows; negative, <9; equivocal, 9 to 11; and positive, >11.
- 2.5. Statistical analysis
- Contingency tables were formed with the antibody titer data measured by the MAT and SAT. Case-by-case associations between the MAT and SAT were estimated by using the Spearman correlation. For this purpose, agglutination units were changed to arbitrary units of stepwise increments. Similarly, the other titers also received higher values. A paired t test was used to obtain the significance of the difference between the MAT and SAT on the individual sample level. The difference in the accumulated titer values obtained from all tested serum samples was compared for the MAT and SAT by general linear model analysis. Comparisons between the SAT and the ELISA were made with the nonparametric Mann-Whitney U test (SPSS v. 11.5, SPSS Inc, Chicago, IL, USA).
2. Materials and Methods
Figure 1.
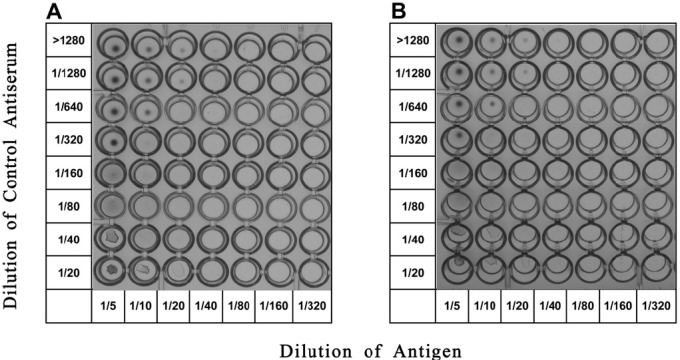
Comparison of titers of commercial Brucella abortus antigens. Block titration of B abortus antigen against the specific, positive control antiserum for each antigen to determine the optimal concentration for use in the microtiter plate. (A) Titration of commercial B abortus (Germaine) against positive control serum (BD). (B) Titration of commercial B abortus (BD) against positive control serum (BD).
- Standardization of antigen concentrations was accomplished in the MAT using each antigen against its specific control antiserum in a block titration (Figure 1). When high concentrations of the antigens were used, the antibody titers were low; conversely, low concentrations of antigen resulted in high antibody titers. As determined by the aforementioned procedure, the optimal concentration of B abortus antigen was ≤1:20, because all combinations of antigen and antiserum dilutions showed complete dispersions of the antigens beyond this point. When the commercial Brucella antigens were diluted 1:10 with saline and compared with OD600, their OD units were 0.76 and 0.79, respectively. The concentrations of the antigens were similar. In the MAT, there were no significant differences in antibody titers against the commercial antigens (Figure 1). The titer of the positive-control serum was 1:160 in the SAT. Ninety sera each were tested by both the SAT and MAT. There were significant differences between the titers obtained using the SAT and MAT with both negative and positive specimens. The SAT was
- Comparisons of sensitivity and specificity between MAT and ELISA
- negative for the 60 healthy sera used as negative controls. There were the same results between the SAT and MAT with the 60 negative specimens. In contrast, all patients presented SAT titers of ≥1:320. In the MAT, each serum was titrated at 3 different antigen dilutions (1:5, 1:10, and 1:20). The results were compared at the individual sample level by testing differences in titers obtained from each concentration (Figure 2). When the antigens were diluted 1:10, the titers were consistent with each other in 16 of the 30 patient sera, while the 13 other sera showed a one phase-titer difference. When the antigens were diluted 1:5, the titers were consistent with each other in 5 sera. When the antigens were diluted at 1:20, the titers were consistent with each other in 9 sera. Thus, the optimal concentration of B abortus antigen in the MAT was 1:10 dilution.
- The results as tested by the SAT, MAT and ELISA is shown in Table 1. When the IgG ELISA results were compared to the MAT results, the sensitivity and specificity of the MAT were 93.3% and 96.7%, respectively. There were 2 false positive and 2 false negative results in the IgG ELISA IgM ELISA results were
- compared to the MAT results, the sensitivity and specificity were 96.7% and 98.3%, respectively. There was one false positive and one false negative result in the IgM ELISA.
3. Results
Figure 2.
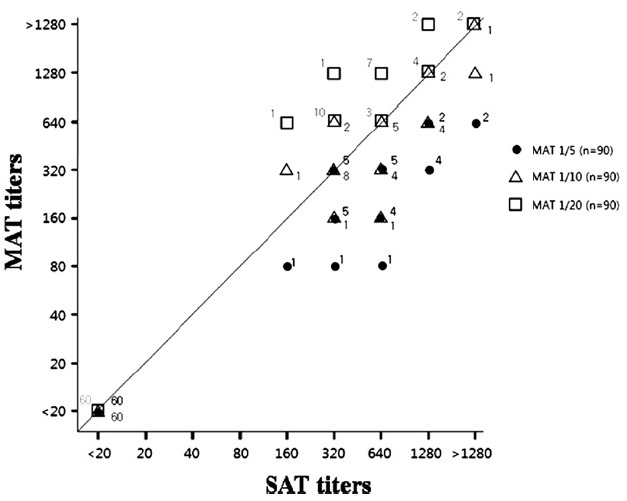
Correlation of agglutination titers as determined by MAT and SAT. The line indicates the same titers in each serologic test. The numbers indicate all samples tested with the each diluted antigen. The symbols distinguish the antigen dilution factor.
Table 1.
Figure 3.

Distribution of ELISA in MAT titers. The concentrations of Brucella IgM (A) or IgG (B) in the <1:20 (negative controls) and the subjects with ≥1:160 are presented as box plots displaying medians and inter quartile ranges. The dotted line indicates the cutoff value for seroactivity to Brucella in ELISA.
- The SAT as a diagnostic tool despite its recognized limitations has led to controversy concerning its clinical implications. The MAT was developed as a simpler and more efficient test than the SAT [9]. However, there have been few studies on the usefulness of the MAT for the diagnosis of domestic human brucellosis. Furthermore, the appropriate concentration of commercial antigens for the MAT has not yet been established.
- In this study, we determined that the optimal concentration of commercial antigens for the MAT is 1:10. The MAT was more specific and sensitive than previously reported and was simpler to perform and the results were easier to read than the SAT.
- ELISAs of IgM and IgG were found to have good agreement compared to the MAT. Disagreement between SAT and ELISA was found in serum samples obtained from both positive and negative patients (Figure 3). There were two false negative results in the IgG ELISA, but these were positive in the IgM ELISA. The reason for this may be that the production of IgG antibody was delayed. There was one false negative result in the IgM ELISA, but it was found to be positive in the IgG ELISA. IgM ELISA has a limited value in the diagnosis of acute brucellosis. Sensitivity increased when the combined IgG and IgM results were compared to agglutination results. The ELISA assay may not have sufficient specificity to be used as a diagnostic tool. The numbers of false positive results in ELISAs of IgG and IgM were two and one, respectively. The reasons for the false-positive results in these specimens remains unclear, and similar results in ELISAs of IgG and IgM have been reported [10,11].
- For the diagnosis of brucellosis, the MAT offered good results, which were in good agreement with those of the ELISA. The results of this study suggest that the MAT may be useful for the diagnosis of brucellosis.
4. Discussion
-
Acknowledgements
- This study was supported by an intramural grant (4837- 300-210-13) from Korea National Institute of Health.
- 1. Pappas G Akritidis N Bosilkovski M et al. Brucellosis. N Engl J Med 2 6 2005;352(22). 2325−36. PMID: 15930423.ArticlePubMed
- 2. Park MY Lee CS Choi YS et al. A sporadic outbreak of human brucellosis in Korea. J Korean Med Sci 12;2005;20(6). 941−6. PMID: 16361801.ArticlePubMedPMC
- 3. Lee K Lim HS Park WW et al. Seroprevalence of brucellosis among risk population in Gyeongsangbuk-do, 2006. J Prev Med Public Health 7;2007;40(4). 285−90. PMID: 17693731.ArticlePubMed
- 4. Franco MP Mulder M Gilman RH et al. Human brucellosis. Lancet Infect Dis 12;2007;7(12). 775−86. PMID: 18045560.ArticlePubMed
- 5. Cobel MJ . Brucellosis in human and animals.. WHO; Geneva: 2006. pp 22−8.
- 6. Araj GF . Update on laboratory diagnosis of human brucellosis. Int J Antimicrob Agents 11;2010;36(Suppl. 1). S12−7. PMID: 20692128.ArticlePubMed
- 7. Welch RJ Litwin CM . A comparison of Brucella IgG and IgM ELISA assays with agglutination methodology. J Clin Lab Anal 2010;24(3). 160−2. PMID: 20486196.ArticlePubMedPMC
- 8. Rose NR Friedman H Fahey JL . Manual of clinical laboratory immunology.. American Society for Microbiology; Washington, D.C: 2006. 3rd ed. pp 385−7.
- 9. Gaultney JB Wende RD Williams RP . Microagglutination procedures for febrile agglutination tests. Appl Microbiol 10;1971;22(4). 635−40. PMID: 5002142.ArticlePubMedPMC
- 10. Gómez MC Nieto JA Rosa C et al. Evaluation of seven tests for diagnosis of human brucellosis in an area where the disease is endemic. Clin Vaccine Immunol 6;2008;15(6). 1031−3. PMID: 18448622.ArticlePubMedPMC
- 11. Moyer NP Evins GM Pigott NE et al. Comparison of serologic screening tests for brucellosis. J Clin Microbiol 10;1987;25(10). 1969−72. PMID: 3117844.ArticlePubMedPMC
Figure & Data
References
Citations
Citations to this article as recorded by 
- The Development of Diagnostic and Vaccine Strategies for Early Detection and Control of Human Brucellosis, Particularly in Endemic Areas
Ayman Elbehiry, Musaad Aldubaib, Eman Marzouk, Adil Abalkhail, Abdulaziz M. Almuzaini, Mohammed Rawway, Ali Alghamdi, Abdullah Alqarni, Mohammed Aldawsari, Abdelmaged Draz
Vaccines.2023; 11(3): 654. CrossRef - New insights into the genetic predisposition of brucellosis and its effect on the gut and vaginal microbiota in goats
Ahmed M. Sallam, Ibrahim Abou-souliman, Henry Reyer, Klaus Wimmers, Alaa Emara Rabee
Scientific Reports.2023;[Epub] CrossRef - Bovine brucellosis – a comprehensive review
Sandip Kumar Khurana, Anju Sehrawat, Ruchi Tiwari, Minakshi Prasad, Baldev Gulati, Muhammad Zubair Shabbir, Rajesh Chhabra, Kumaragurubaran Karthik, Shailesh Kumar Patel, Mamta Pathak, Mohd. Iqbal Yatoo, Vivek Kumar Gupta, Kuldeep Dhama, Ranjit Sah, Wanpe
Veterinary Quarterly.2021; 41(1): 61. CrossRef - Microbiological Laboratory Diagnosis of Human Brucellosis: An Overview
Giovanni Di Bonaventura, Silvia Angeletti, Andrea Ianni, Tommasangelo Petitti, Giovanni Gherardi
Pathogens.2021; 10(12): 1623. CrossRef - The spatiotemporal distribution of human brucellosis in mainland China from 2007-2016
Peifeng Liang, Yuan Zhao, Jianhua Zhao, Dongfeng Pan, Zhongqin Guo
BMC Infectious Diseases.2020;[Epub] CrossRef - Brucellar spondylodiscitis: A case series with focus on histopathological features
Soumaya Rammeh, Emna Romdhane, Hend Riahi, Meriem Ksentini, Mouna Chelli Bouaziz, Rahma Ayadi, Aida Berriche, Yosra Chebbi, Mohamed Fethi Ladeb
Journal of Clinical Neuroscience.2020; 78: 360. CrossRef - A case report of neurobrucellosis mimicking Guillain–Barré syndrome
Parastoo Paydarnia, Soroush Moradi, Arman Habibi, Ladan Abbasian, Mojdeh Ghabaee
Neurology, Psychiatry and Brain Research.2019; 31: 27. CrossRef - A compact laser diode based photoacoustic spectral response technique to differentiate Brucellosis infected goat tissue from normal tissues
A. Gorey, S. Shukla, J.G. Prasad, S. Verma, A. Sharma, S. Vasudevan
Journal of Instrumentation.2019; 14(05): P05017. CrossRef - Laboratory Diagnosis of Human Brucellosis
Pablo Yagupsky, Pilar Morata, Juan D. Colmenero
Clinical Microbiology Reviews.2019;[Epub] CrossRef - Real-time PCR assays for diagnosing brucellar spondylitis using formalin-fixed paraffin-embedded tissues
Man Li, Xingang Zhou, Jingjing Li, Lei Sun, Xiangmei Chen, Peng Wang
Medicine.2018; 97(9): e0062. CrossRef - Incidence of human brucellosis in the Kilimanjaro Region of Tanzania in the periods 2007–2008 and 2012–2014
Manuela Carugati, Holly M Biggs, Michael J Maze, Robyn A Stoddard, Shama Cash-Goldwasser, Julian T Hertz, Jo E B Halliday, Wilbrod Saganda, Bingileki F Lwezaula, Rudovick R Kazwala, Sarah Cleaveland, Venance P Maro, Matthew P Rubach, John A Crump
Transactions of The Royal Society of Tropical Medi.2018; 112(3): 136. CrossRef - Seroreactivity and Risk Factors Associated with Human Brucellosis among Cattle Slaughterhouse Workers in South Korea
Dilaram Acharya, Seon Hwang, Ji-Hyuk Park
International Journal of Environmental Research an.2018; 15(11): 2396. CrossRef - Outbreak of human brucellosis in Southern Brazil and historical review of data from 2009 to 2018
Tamilly Silva Lemos, Juliana Clelia Cequinel, Tania Portela Costa, Amanda Boni Navarro, Andressa Sprada, Flávia Kazumi Shibata, Regina Gondolfo, Felipe Francisco Tuon, Stephen Baker
PLOS Neglected Tropical Diseases.2018; 12(9): e0006770. CrossRef - Brucellosis in Immunocompromised Hosts
KA Al-Anazi, AM Al-Jasser
Archives of Organ Transplantation.2016; 1(1): 001. CrossRef - Evaluation and Selection of Multilocus Variable-Number Tandem-Repeat Analysis Primers for Genotyping Brucella abortus Biovar 1 Isolated from Human Patients
Subok Lee, Kyu-Jam Hwang, Mi-Yeoun Park, Seon-Do Hwang, Hee-Youl Chai, Hyuk Chu, Sang-Hee Park
Osong Public Health and Research Perspectives.2013; 4(5): 265. CrossRef
 PubReader
PubReader Cite
Cite


