
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 3(3); 2012 > Article
-
Articles
JXTA: A Technology Facilitating Mobile P2P Health Management System - Rajasekaran Rajkumar, Narayana Iyengar Nallani Chackravatula Sriman
-
Osong Public Health and Research Perspectives 2012;3(3):165-169.
DOI: https://doi.org/10.1016/j.phrp.2012.04.008
Published online: June 30, 2012
School of Computer Science and Engineering, Vellore Institute of Technology University, Vellore, India.
- Corresponding author. E-mail: rrajkumar@vit.ac.in
Copyright ©2012, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License () which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- Mobile JXTA (Juxtapose) gaining momentum and has attracted the interest of doctors and patients through P2P service that transmits messages. Audio and video can also be transmitted through JXTA. The use of mobile streaming mechanism with the support of mobile hospital management and healthcare system would enable better interaction between doctors, nurses, and the hospital. Experimental results demonstrate good performance in comparison with conventional systems. This study evaluates P2P JXTA/JXME (JXTA functionality to MIDP devices.) which facilitates peer-to-peer application+ using mobile-constraint devices. Also a proven learning algorithm was used to automatically send and process sorted patient data to nurses.
-
Methods
- From December 2010 to December 2011, a total of 500 patients were referred to our hospital due to minor health problems and were monitored. We selected all of the peer groups and the control server, which controlled the BMO (Block Medical Officer) peer groups and BMO through the doctor peer groups, and prescriptions were delivered to the patient’s mobile phones through the JXTA/ JXME network.
-
Results
- All 500 patients were registered in the JXTA network. Among these, 300 patient histories were referred to the record peer group by the doctors, 100 patients were referred to the external doctor peer group, and 100 patients were registered as new users in the JXTA/JXME network.
-
Conclusion
- This system was developed for mobile streaming applications and was designed to support the mobile health management system using JXTA/ JXME. The simulated results show that this system can carry out streaming audio and video applications. Controlling and monitoring by the doctor peer group makes the system more flexible and structured. Enhanced studies are needed to improve knowledge mining and cloud-based M health management technology in comparison with the traditional system.
- Peer to peer is not a centralized system but the client server status is available in the network. Here, a patient node in the network resembles a peer, but equal or highpriority statuses can be applied, and referents to the peer service can be requested or issued. All peer groups, except the control peer group, have equal status but they are not necessarily equal in terms of physically available. When comparing P2P with the client server, P2P is considered active or alert if at least one node is active. When no peers are live, the network is unavailable. The possibility of using P2P applications on mobile devices are presented in this report, including a message-passing application and a file-sharing application. The open source JXTA/JXME framework is also presented here. In P2P systems, every peer contributes and takes advantage of the information made available by other peers. The peer control nodes are individual decision makers that act in a rational and demanding way, but they are not liable and cooperation will happen when the appropriate economic and social mechanisms demonstrate failure. P2P system performance is poor only when fewer peers offer services and a solution is needed. More P2P applications are beginning to be adopt that can balance policies that target equivalence and compare the donation and saving of individual peers, e.g., the mule’s auction or system. In the present scenario, the P2P models were widely used to transfer and share files. JXTA is a collaborative approach for peer-to-peer computing, and a strong need exists for variety of applications. JXTA is spontaneous, selforganized, and provides more effective service than a single centralized server, scalable robustness, dynamic behavior, and spontaneity. When exchanging data among peers in a closed group, the two main things that must be considered are security and authentication. Hoping that these could be resolved using the JXTA/ JXME framework, the architecture of the mobile P2P hospital management and health care system using JXME (the mobile version of JXTA) is proposed in this paper. This provides an attractive and generic infrastructure that can rapidly define and implement custom peer-to-peer services. The potential of the P2P architecture, which includes a distributed environment and P2P mobile JXTA, will be fully explored in the coming years. Our paper describes an approach for developing mobile healthcare applications in the P2P environment.
- 1.1. P2P JXTA Protocols
- A variety of protocols, architectures, and implementations that can analyze the results of existing P2P solutions already exist. To design P2P applications, developers often use diverse methodologies. All of these are asynchronous and based on the query-response model. Using these protocols, peers can discover each other or network resources. Peers are not required to implement all of the protocols; instead, they just implement what they need. JXTA protocols have been used as the foundation for building mobile-commerce applications. They resemble and identify poor overhead protocols to analyze low-level network topology. The identification of various protocols that could be used in the JXTA framework with various functionalities is analyzed here. We considered the peer-membership protocol (PMP) when using the JXTA framework.
- A peer is included in the PMP when joining or leaving a peer group. PMP identifies the methods accessed by the peers, and JXTA network sends the appropriate message to hospital management.
- New membership requests can be applied to the authenticator if a peer is interested in joining the group. A response message or an acknowledgement is sent back by the authenticator to the peer as a form.
- An addition is added to the record after application. The peer selects addition to the peer group.
- Updating is performed by the recorded peer group. Patient records change after consultations with doctors. A message is sent to the patient to update membership information if this change is needed.
- An authenticator can reject peer membership. PMP is used by the architecture in order to allow a peer to join a peer group.
- Creates groups and publishes advertisements. The abovementioned architecture advertisement ADVT protocol also provides code for membership policies. Thus, authentication and authorization can be achieved using this protocol. By using this protocol, any peer (i.e., user) can automatically change the group identification by leaving the present group and joining another new group. In this case, any peer in the proxy group can leave that group by using the “finish” command and join another group, which is then designated as proxy group 2.
1. Introduction
1.1.1. Peer-membership protocol
1.1.2. Patient request
1.1.3. Addition
1.1.4. Modifications and update
1.1.5. Rejection
1.1.6. PMP functionality
- The permanent Internet Protocol networks that are used for streaming are different from mobile IP networks. The mobile JXTA network has a streaming technique that is of good quality and has no service delays. Streaming and messaging work in real time, but its limitation is storage space. The streaming service needs at least a media server and a streaming client. The P2P message server holds all of the information related to SMS, MMS, doctors, and patients. Added components, such as the presentation and caching server, are used to provide additional services in order to improve the overall quality of services.
- The registration peer (Pr1, Pr2 ) is responsible for registering new patients who enter the peer group using their mobile phone. Regular users or users whose entry is given by the doctors are entered into the peer group and identified as Pid1, Pid2...Pidn. If the nurse needs to know the history of the patient, the recorded peer group holds all of the information about the registered patient, and all of the past history and necessary information is made available to the peer group. The nurses in the nurse peer group can identify the patient and send doctors in the doctor peer group. The BMO peer center (M2) is responsible for monitoring the recorded peer group and monitoring and controlling the doctor peer group. The doctors and nurses inside the peer group are responsible for giving treatment to registered patients, and M2 is in control of the two peer groups. The server provides tutorials and guidance to the nurses via audio and video files. The nurse can request data using the JXTA network and retrieve data using the streaming technique. This method can help nurses administer treatments suggested by the doctor inside the peer group. The pharmacist peer group is responsible for delivering prescriptions to the patient through SMS. The M1 peer control, which is responsible for the number of BMO peers and controls, monitors all of the peer groups within a JXTA network. If the nurse needs to know the history of the patient, the server provides tutorials or guidance to the nurse in the form of audio and video files. The nurse can request data using SMS and retrieve data using the streaming technique. This method helps nurses administer the treatments suggested by the doctor.
- 2.1. Simulation of the Proposed System
- As previously discussed there are wearable sensors that can measure body temperature, pulse rate, respiration rate, oxygen level in blood (SpO2), BIS, and ECG. These readings can be sent to the patient’s mobile device via a wireless communication channel. These data can be messaged to the recorded peer group via the JXTA framework, as shown in Figure 1. J2ME processing of the recorded peer group can classify these sets of readings as “normal” or “critical.” Dual-weight learning vector quantization has a low computational complexity and a high recognition rate.
- Dual-weight learning vector quantization Algorithm:
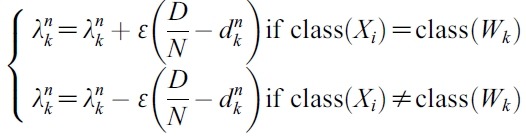
1. If we have n types of readings available from the wearable sensors, we can use n-dimensional training vectors (x1, x2, .. xn ) to analyze them. It is easy to obtain a set of such readings and the corresponding outputs from patient records. Select some of these input vectors as the reference vector “W.” The remaining vectors are training vectors “X.” Initialize the importance vector λ ( = 1/n ) for each W, learning rates (α and ε), and the maximum number of iterations.
2. If the maximum number of iteration is reached, then stop; otherwise, continue.
3. For an arbitrary training vector Xi, find the nearest reference vector Wm using the following formula:
- Distance between Xi and
- and
- δwhere D = the distance between Xi and Wk,
- and δ is a predefined threshold such that (0 < δ < 1/n).
- Once the sensor readings are classified, they are sent to nurse peer group associated with the patient. The nurse can request information from BMO (M2) regarding the availability of doctors, as well as their years of experience, and if the situation is critical a highly experienced doctor can be requested. This expedites the whole process. The nurse can immediately know if there is a potentially serious condition developing in a patient. Appropriate precautions can be taken in advance in such cases.
- 2.2. Sample Peer Group Advertisement
- Advertisement impose hierarchal elements on the proposed system peer group, and advertisements are followed that describe peer group-specific recourses such as service name, group identification, service description, patient specification, and service parameters. A sample advertisement is given; a new group can be created using different identification numbers from different groups. The name of the new group is reported and the same description is made regarding the group. Thus, a peer group advertisement is created. Any advertisement that comes to this group passes the message to its many identifiers; for example, a free checkup camp can be proposed by the hospital and organized by the doctor peer group, and a message can be passed to all of the registered patients (Figures 2 and 3).
2. Materials and Methods







- Five hundred patients were monitored during the study period, and their records were maintained. Three hundred referred patient records and 100 patients were referred to the specialists, i.e., the external doctor peer group, and 100 new users were registered and new information was gathered regarding them (Table 1).
3. Results
- In existing telemedicine systems, various methods have been developed for streaming applications for use in mobile systems that use MMS or SMS that help diagnose disease without the presence of a physician [1,14]. A decision-making support system that uses smart mobile devices in a telemedicine system could raise the quality of the medical services and also provide patients with routine information concerning consultation with physicians. This approach has many advantages, and accuracy improves the quality of service of hospital operations [2,13]. In the discovery approach, classification is integrated for both context awareness and semantic-based matchmaking; however, this model lacks service announcements, service descriptions, service roaming, and service registration [3,12]. Integration of a mobile healthcare system for delivering primary medical care to the rural residents of India. This system was envisioned as being hospital based in order to provide medical services to enrolled members through a healthcare cooperative that was established using regional, rural, electric sensors and by integrating wireless sensors and personal body area network into an intelligent mobile health monitoring system with input from patients [4,10]. The doctors do not have to stay at the hospital where they use MMS technology and the telemedicine system. Management software is used to evaluate performance between the medical center and the disaster areas with the help of mobile networks;
- Patients and their peer groups
- however, the drawback is that patients are unable to communicate during emergencies [5]. A mobile P2P was realized that used JXTA in a hospital environment where patient data were electronically stored [6]. The virtual storage system of the patient records history is not maintained [6,11]. Body sensors are implemented to find the emergency situations and take the necessary actions [7]. Geographic spatial data from anywhere is possible, but security issues are a large problem in these processes [8]. A telemonitoring or tele treatment is done for patients on the request to the doctors false treatments have more chances [9].
4. Discussion
| Month | No. of patients | Referred recorded peer group | External peer group | New users |
|---|---|---|---|---|
|
|
||||
| Dec 10– Mar 11 | 120 | 70 | 25 | 20 |
| Apr 11– Jul 11 | 230 | 120 | 62 | 40 |
| Aug 11 –Dec 11 | 150 | 110 | 13 | 40 |
- This system was developed for mobile streaming applications and was designed to support the mobile health management system using JXTA/JXME. The simulated results show that this system can carry out streaming audio and video applications. Controlling and monitoring by the doctor peer group makes the system more flexible and structured. Enhanced studies are needed to improve knowledge mining and cloud-based M health management technology in comparison with the traditional system.
5. Conclusion
- 1. Dasgupta A. . A framework for mobile based geospatial public health management, in Students Technology Symposium (Tech- Sym).. IEEE; 2010. pp 82−87.
- 2. Kim J Kim D Jung S et al.. Implementation and performance evaluation of mobile ad hoc network for emergency telemedicine system in disaster areas. Engineering in Medicine and Biology Society In: EMBC 2009. Annual International Conference of the IEEE.; 2009. p. 1663−1666.
- 3. Kranen P Muller E Seidl T et al.. Mobile mining and information management in Health Net Scenarios. Mobile Data Management In: MDM ’08. 9th International Conference.; 2008. p. 215−216.
- 4. Lee CN Chu YT Cheng L. . Usage of smart mobile device at the telemedicine. Machine Learning and Cybernetics (ICMLC) In: International Conference; 2011. p. 582−587.
- 5. Lim H Choi S. . Design and implementation of iSCSI-based virtual storage system for mobile health care. Enterprise networking and computing in healthcare industry In: HEALTHCOM 2005. Proceedings of 7th International Workshop.; 2005. p. 37−40.
- 6. Lu SH Lai KC Yang DL et al.. Pervasive health service system: insights on the development of a grid-based personal health service system. e-Health Networking Applications and Services (Healthcom) In: 12th IEEE International Conference; 2010. p. 61−67.
- 7. Maibaum N Mundt T. . JXTA: A technology facilitating mobile peer-to-peer networks. In: Mobility and Wireless Access Workshop, MobiWac 2002. International.; 2002. p. 7−13.
- 8. Setyono A Alam M Eswaran C. . Development of streaming application for mobile telemedicine system using multimedia messaging service technology. Communication Software and Networks (ICCSN) In: IEEE 3rd International Conference.; 2011. p. 574−578.
- 9. Shin D. . m-healthcare revolution: an e-commerce perspective. Computers, Networks, Systems and Industrial Engineering (CNSI) In: First ACIS/JNU International Conference; 2011. p. 105−106.
- 10. Sukanesh R Rajan S Vijayprasath S et al.. Intelligent wireless mobile patient monitoring system. Communication Control and Computing Technologies (ICCCCT) In: IEEE International Conference; 2010. p. 540−543.
- 11. Toninelli A Montanari R Corradi A. . Enabling secure service discovery in mobile healthcare enterprise networks. Wireless Communications IEEE 2009;16(3). 24−32.Article
- 12. Wac K Bults R van Beijnum B et al.. Mobile patient monitoring: the MobiHealth system. Engineering in Medicine and Biology Society In: EMBC 2009. Annual International Conference of the IEEE.; 2009. p. 1238−1241.
- 13. Yan H Huo H Xu Y et al.. Wireless sensor network based Ehealth system implementation and experimental results. Consumer Electronics IEEE Transactions 2010;56(4). 2288−95.Article
- 14. Zhou F Cheng F Wei L et al.. Cloud service platform–hospital information exchange (HIX). e-Business Engineering (ICEBE) In: IEEE 8th International Conference; 2011. p. 380−385.
Figure & Data
References
Citations
- Optimal mobile device selection for round-robin data exchange via adaptive multi-criteria decision analysis
Young-Long Chen, Chih-Kun Ke
Computers & Electrical Engineering.2016; 54: 119. CrossRef - An Optimal Mobile Service for Telecare Data Synchronization using a Role-based Access Control Model and Mobile Peer-to-Peer Technology
Chih-Kun Ke, Zheng-Hua Lin
Journal of Medical Systems.2015;[Epub] CrossRef
 PubReader
PubReader Cite
Cite


