
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 3(2); 2012 > Article
-
Articles
Epidemiological and Immunological Characteristics at the Time of HIV Diagnosis for HIV/AIDS Cohort Registrants Representative of HIV-Infected Populations in Korea - Jin-Hee Lee, Seung Hyun Kim, Jin-Sook Wang, Kyoung Mi Sung, Sung Soon Kim, Mee-Kyung Kee
-
Osong Public Health and Research Perspectives 2012;3(2):100-106.
DOI: https://doi.org/10.1016/j.phrp.2012.04.002
Published online: June 30, 2012
Division of AIDS, Korea National Institute of Health, Osong, Korea.
- 1These authors equally contributed to this work.
- 1These authors equally contributed to this work.
- *Corresponding author. E-mail: keemk60@yahoo.co.kr
Copyright ©2012, Korea Centers for Disease Control and Prevention
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License () which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- The Korea HIV/AIDS cohort was constructed with 18 hospitals that care for HIV-infected individuals in 2006. We compared the epidemiological and immunological characteristics of the cohort registrants with those of the HIVinfected population at the time of HIV diagnosis.
-
Methods
- This study was conducted on 5717 people living with HIV/AIDS from 1985 to 2009, of which 789 individuals registered with the Korea HIV/AIDS cohort study. Individuals who had data from initial CD4+ T-cell counts measured within 6 months following HIV diagnosis were selected as study participants to predict the status of disease progression at the time of HIV diagnosis. A total of 2886 patients (50%) were selected from people living with HIV/AIDS, of whom 424 individuals (54%) were cohort registrants. The χ2 test and Wilcoxon rank sum test were used for analysis.
-
Results
- The distributions of age, marital status, diagnosed regions, reason for HIV testing, and screening site were similar between the HIV-infected population and the cohort registrants. In 1985–2004, the male ratio for the cohort registrants (94.3%) was significantly higher than that measured for the HIV-infected population (89.5%) (p = 0.0339). With regard to transmission route, homosexual contact of cohort registrants (46.6%) was higher than that of the HIV-infected population (40.1%) (p = 0.022) in 2005–2009. No statistical difference in CD4+ T-cell counts at the time of HIV diagnosis was found between the HIVinfected population and cohort registrants (p = 0.2195).
-
Conclusion
- The Korea HIV/AIDS cohort registrants represent the HIV-infected population, and the data collected from this cohort could be used as a foundation for national statistics.
- Since the first HIV infection was discovered in 1985, a total of 8535 HIV-infected individuals have been identified as of the end of December 2011, and 7032 people living with HIV/AIDS (PLWHA, 82%) of those infected are in Korea [1]. Recently, approximately 700–800 HIV-infected individuals have been identified each year, and it is expected that the number of PLWHA will exponentially increase in the future. HIV infection causes lifelong loss cost of approximately US$400,000 per individual, causing both personal and national socioeconomic burdens [2]. Therefore, it is important to develop strategies to prevent HIV infection.
- In Korea, HIV-infected individuals have been managed by the government according to the HIV Prevention Act. In addition, the national and local governments support the cost associated with AIDS treatment and HIV-related tests. However, clinical information and treatment data obtained are managed by hospitals, whereas their diagnostic and epidemiologic data are managed by the Korea Centers for Disease Control and Prevention (KCDC). Thus, the national statistics calculated by integrating the data from HIVinfected individuals and the utilization of relevant information for HIV/AIDS research have been limited. In addition, as the protection of individual privacy has been increasingly emphasized since the enforcement of the Bioethics and Safety Act in 2005, it has become mandatory to obtain informed consent forms from participants when samples and data from the participants are collected for HIV/AIDS research [3].
- In developed countries, the HIV/AIDS cohort has been in existence since the 1980s, allowing for significant outcomes in the areas of HIV diagnostic technology, treatment, and other researches [4-7]. In particular, the Swiss HIV Cohort Study (SHCS) is an open cohort in which HIV-infected individuals are continuously registered as participants [5]. Forty-five percent of the total Swiss HIV-infected individuals and 69% of AIDS patients are registered as SHCS participants, allowing for the results of the cohort studies to be directly utilized for the control of national policies on HIV/AIDS prevention. With reference to the SHCS, the KCDC constructed the Korea HIV/AIDS cohort with 18 hospitals that care for HIV-infected individuals in 2006 [9]. Cohort registrants are recruited among HIV-infected individuals over 18 years old who undergo treatments in the aforementioned hospitals. A follow-up is conducted every 6 months, and the blood samples and relevant data from the registrants are sent to the KCDC. Since the establishment of the Korea HIV/AIDS cohort study, approximately 850 HIV-infected individuals have been registered to the cohort during a 5-year period (2007– 2011). A basic study for correcting and minimizing bias is required before utilization of the data and samples from the cohort study and the application of the results to future HIV/AIDS prevention polices. Moreover, when recruiting new registrants to the open cohort, basic data are needed to adjust for the representation of the cohort registrants for the HIV-infected population upon registration to the cohort. For these reasons, we compared the epidemiological and immunological characteristics of the cohort registrants with those of the HIV-infected population at the baseline, which is the time of HIV diagnosis.
1. Introduction
- 2.1. Subjects
- If an individual is diagnosed with an HIV infection through the national HIV surveillance system in Korea, it is reported to the KCDC. The KCDC conducts an HIV epidemiologic survey through public health centers and manages the collected data via the HIV database(DB) system. In addition, the KCDC conducts immunological tests to assess the progression status of the disease when patients are diagnosed with HIV infection, and manages the results with the HIV laboratory information management system (LIMS) [8].
- This study was conducted on 5717 PLWHA from a total of 6883 HIV-diagnosed individuals who have been registered from 1985 to 2009, of whom 789 individuals registered with the Korea HIV/AIDS cohort study. We defined 5717 PLWHA as the HIV-infected population in this study. Individuals who had data from the initial CD4+ T-cell count measured within 6 months after the diagnosis of HIV infection were selected as participants to predict the status of disease progression at the time of HIV diagnosis. A total of 2886 patients (50%) were selected among PLWHA, of whom 424 individuals (54%) were cohort registrants.
- 2.2. Statistical analysis
- The following variables were compared between the HIV-infected population and the Korea HIV/AIDS cohort registrants using epidemiological data and the CD4+ T-cell counts managed by the HIV DB system and the HIV laboratory information system in KCDC, respectively: gender, age, transmission route, marital status, diagnosed region, screening site, reason for HIV testing, and diagnosed year for HIV infection.
- The proportion of HIV/AIDS cohort registrants for the HIV-infected population by year of diagnosis is shown in Table 1. Because we registered the Korea HIV/AIDS cohort participants from 2007 and tried to recruit recently diagnosed individuals, the HIV-infected individuals after the diagnosed year of 2005 were actively registered in the Korea HIV/AIDS cohort (Table 1). For this reason, we compared the characteristics of those who belong to the HIV-infected population and the cohort registrants by dividing them into two groups: 1985–2004 and 2005–2009.
- Distribution of the HIV-infected population and the Korea HIV/AIDS cohort registration by year of HIV diagnosis
- With regard to individuals age, the age at the time of HIV diagnosis was used. As for marital status, divorce or separation by death at the time of HIV diagnosis was classified as married. For the diagnosed regions, seven big cities and the remaining areas were classified into metropolitan cities and small towns or rural areas, respectively. Screening sites were classified into three groups: public institutions, hospitals, and blood banks. For HIV transmission routes, sexual contact were classified into two groups: heterosexual and homosexual. Infection by blood transfusion or blood products and mother-to-child transmission were classified as others. For reason for HIV testing, reasons at the time of HIV screening were used, which followed the classification criteria of a previous study [10].
- To compare the epidemiological characteristics of the cohort registrants with the HIV-infected population by the year of HIV diagnosis, χ2 test was conducted for each epidemiologic variable. To compare the status of disease progression at the time of HIV diagnosis, Wilcoxon rank sum test was performed for the difference in measured CD4+ T-cell counts. A significance level of 0.05 was used for statistical testing, and results were analyzed using the SAS 9.1 version software.
2. Materials and Methods
- 3.1. Epidemiological characteristics of HIV-infected populations and of HIV/AIDS cohort registrants
- The epidemiological characteristics of HIV-infected population are presented in Table 2. Approximately 92% of the HIV-infected population was male, and individuals in the 30s accounted for the largest population (32.2%). The transmission route was mainly caused by sexual contact; heterosexual contact (59.3%) was higher than homosexual contact (40.1%). As for marital status, unmarried individuals (62.5%) accounted for a larger percentage of the study individuals (married individuals comprised 37.5%). As for the diagnosed region, metropolitan cities (69.6%) accounted for the higher percentage of individuals than those reported for small towns and rural areas (30.4%). The individuals were diagnosed with HIV testing for clinical manifestation (39.4%), health checkup (26.8%), and knowledge of status (14.2%). The hospital accounted for the largest portion (68%) of screening sites, followed by public institution (22.2%).
- Comparison of epidemiological characteristics, wherein individuals were divided into two groups according to the year of diagnosis, demonstrated differences in gender, age, reason for HIV testing, and screening site. Compared with the 1985–2004 group, the both percentages of males and the older age of HIV diagnosis are higher in the 2005–2009 group. In addition, clinical manifestation is the major reason for initial HIV testing, and voluntary testing for knowledge of status accounted for a larger percentage in the 2005–2009 group compared to the 1985–2004 group.
- Table 3 compares the epidemiological characteristics of the cohort registrants and the HIV-infected population. The distributions including age, marital status, diagnosed region, reason for HIV testing, and screening site were similar between the HIV-infected population and the cohort registrants. The HIV-infected population in 1985–2004 is 40.7% (2326 individuals) of the total, while that of cohort registrants is lower (33.8%, 267 individuals), and the male was significantly higher in the cohort registrants (94.3%) than in the HIV-infected population (89.5%) (p = 0.0339). However, for the transmission route, homosexual contact in the cohort registrants (46.6%) was higher than that of the HIVinfected population (40.1%) from 2005 to 2009 (p = 0.022).
- Comparison of epidemiological characteristics of the HIV-infected population by year of HIV diagnosis
-
1Others: Infection by blood transfusion or blood products, and mother to child transmission; 2Married: Include divorce or separation by death at the time of HIV diagnosis; 3Reason for HIV test: Reasons at the time of HIV screening.
-
HIV-infected population: People living with HIV/AIDS from 1985 to 2009.
- 3.2. Immunological characteristics of the HIV-infected population and of HIV/AIDS cohort registrants
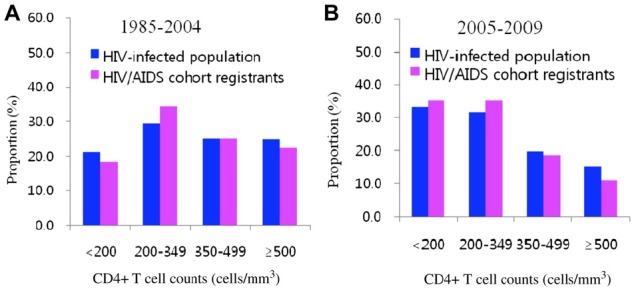
- The median value of CD4+ T-cell counts for the cohort registrants during 1985–2004 (348 cells/mm3, interquartile range: 225–496) was statistically higher than that in the 2005–2009 group (275 cells/mm3, interquartile range: 160–413) (p < 0.0001; data not shown). The comparison of the distribution of CD4+ T-cell counts at the time of HIV diagnosis between the HIV-infected population and the cohort registrants are presented in Figure 1. Meanwhile, as compared to the immune level distribution of the HIV-infected population, the cohort registrants in the 1985–2004 group showed a higher level (200–349 cells/mm3), although no statistical significance was found between two groups (p = 0.5732). In addition, the cohort registrants in the 2005–2009 group exhibited increased levels, <200 and 200–349 cells/mm3, than the HIV-infected population; however, no statistical significance was found between two groups (p = 0.2195).
3. Results
- The Joint United Nations Programme on HIV/AIDS has estimated that, since the first HIV case was reported in 1981, the number of PLWHA has reached 33.3 million (31.4–35.3 million) by the end of 2009. The male to female ratio of HIV-infected individuals is almost 1:1, and individuals aged younger than 15 years accounted for 7% of the total [11].
- Comparison of the epidemiological characteristics of the Korea HIV/AIDS cohort registrants with the HIV-infected population by the year of HIV diagnosis
-
*HIV-infected population: HIV-infected population: people living with HIV/AIDS from 1985 to 2009; 1Others: Infection by blood transfusion or blood products, and mother to child transmission; 2Married: include divorce or separation by death at the time of HIV diagnosis; 3Reason for HIV test: Reasons at the time of HIV screening.
- In Korea, the number of HIV-infected individuals has continuously increased, and more than 700 infected individuals have recently been diagnosed every year. Most HIV-infected Koreans are male (male to female ratio 11:1), of whom more than 99% received HIV through sexual contact. Majority of infected individuals have been diagnosed through HIV testing due to clinical manifestation, and in agreement with a previous study [10]. The incidence of late diagnosis has steadily increased. In addition, the proportions of males and of older age at diagnosis have also rised.
- So far, HIV prevalence has been low [12], but the number of PLWHA in Korea has reached a total of more than 7000 as of 2011. Therefore, AIDS prevention policies including the reduction of HIV transmission, and the promotion of a healthy lifestyle for HIV-infected individuals have been increasingly required. Accordingly, the Korean government has managed various programs including the early diagnosis of HIV infection, support for the treatment of HIV-infected individuals, and counseling. However, for the establishment and evaluation of HIV prevention policies efficiently, scientific evidence is required.
- For example, in the US, the Multicenter AIDS Cohort Study (1984) for male homosexuals and the Women’s Interagency HIV Study (1994) for female heterosexuals have already been established [13,14]. The results of the HIV/AIDS cohort studies were applied to national programs for HIV prevention as well as to diagnostic and treatment guidelines for HIV-infected individuals, and the development of therapeutic drugs, thereby extending the survival of infected individuals and preventing the transmission of HIV infection [15,16]. In Europe, the multinational cohort, Concerted Action on SeroConversion to AIDS and Death in Europe (1997), in which 12 countries participated, was established for individuals whose HIV infection time can be predicted [17].
- In Korea, HIV prevalence was very low and the pool of HIV researchers was also small before 2000. Thus, the HIV studies representing the HIV-infected population, such as survival rate, therapeutic effects, and clinical characteristics were insufficient. However, as the number of HIV-infected individuals has increased since 2000, the Korea HIV/AIDS cohort study was established in 2006 to obtain basic data that can be applied to the establishment of preventive policies based on scientific evidence and to construct an infrastructure that promotes HIV/AIDS studies under the system that financially supports HIV-infected individuals.
- In this study, we evaluated whether the cohort registrants represent the HIV-infected population. The results demonstrate that gender and transmission routes are different from the HIV-infected population. Before 2005, the percentage of males is higher in cohort registrants than in the HIV-infected population. This is a direct result of the different distribution of the diagnosed year in the cohort registrant and the recently increased proportion of males in the HIV-infected population in Korea. In particular, the major transmission route of recently identified infected individuals was homosexual contact, which is higher than that reported for the HIV-infected population.
- Following the results of HIV epidemiologic survey, the male to female ratio of the HIV-infected population is 11:1, and the proportion of those infected through heterosexual contact is steadily higher than that of homosexual contact. However, the answer to the transmission route was occasionally changed in the next survey, and an accurate analysis is required for the survey regarding the route of transmission. The comparison of the CD4+ T-cell counts at the time of HIV diagnosis between HIV-infected population and the cohort registrants indicated that the progression of HIV is similar between the two groups.
- In addition, the results for the comparison of the time taken to register with the cohort study after the HIV diagnosis demonstrated that the cohort registration proportion was 30% and 57% within 1 and 3 years after the diagnosis of HIV infection, respectively (Table 4). As soon as the infected individuals are diagnosed, they
- Time interval between the cohort registration and the HIV diagnosis of Korea HIV/AIDS cohort registrants
- are treated in the hospital according to the guideline established for HIV/AIDS in recent years [1]. Therefore, the period between the HIV diagnosis and cohort registration will be decreased.
- No significant difference in the epidemiological and immunological criteria was found between the HIVinfected population and cohort registrants. Our results indicated that the Korea HIV/AIDS cohort registrants represent the HIV-infected population, and that the data collected from this cohort can be used as a foundation for national statistics. We also suggest that selection bias in the cohort study should be checked continuously for the maintenance of a representative sampling.
4. Discussion
Comparison of CD4+ T-cell counts at the time of HIV diagnosis between the HIV-infected population and Korea HIV/AIDS cohort registrants in (A) 1985–2004 and (B) 2005–2009.
| Periods (year) | Frequency | Percentage |
|---|---|---|
|
|
||
| ≤1 year | 244 | 30.9 |
| 1-3years | 215 | 27.3 |
| 4-5years | 132 | 16.7 |
| 6-10 years | 147 | 18.6 |
| >10 years | 51 | 6.5 |
-
Acknowledgements
- This study was supported by a grant from the Chronic Infections Disease Cohort Study (4800-4859-304-210) and from the Korea Centers for Disease Control and Prevention.
- 1. Korea Centers for Disease Control and Prevention.Guideline for HIV/AIDS Control. KCDC; 2012. pp 14−17.
- 2. KCDC and UNDP, Korea.The Social and Economic Impacts of HIV/AIDS Infection in Korea, The Report of International AIDS Symposium 2004;177−189.
- 3. Ministry for Health Welfare and Family Affairs.Information field: The data of laws. Bioethics..
- 4. Thierfelder C Weber R Elzi L et al. Participation, characteristics and retention rates of HIV-positive immigrants in the Swiss HIV Cohort Study. HIV Med 2;2012;13(2). 118−26. PMID: 22107170.ArticlePubMed
- 5. Swiss HIV.Cohort study. Cohort profile: the Swiss HIV Cohort Study. Int J Epidemiol 10;2010;39(5). 1179−89. PMID: 19948780.ArticlePubMed
- 6. Collaborative Group on AIDS Incubation.Time from HIV-1 seroconversion to AIDS and death before widespread use of highlyactive antiretroviral therapy: a collaborative re-analysis. Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Concerted Action on SeroConversion to AIDS and Death in Europe. Lancet 2000;355:1131−7. PMID: 10791375.ArticlePubMed
- 7. CASCADE Collaboration.Differences in CD4 cell counts at seroconversion and decline among 5739 HIV-1 infected individuals with well-estimated dates of seroconversion. J Acquir Immune Defic Syndr 9;2003;34(1). 76−83. PMID: 14501798.ArticlePubMed
- 8. Korea Centers for Disease Control and Prevention.Guideline for HIV/AIDS Control. KCDC; 2012. pp 81−115.
- 9. Kee MK Wang JS Kim SH et al. The profile of Korea HIV/AIDS Cohort Study, The 10th International Congress on AIDS in Asia and the Pacific. Republic of Korea; Busan: 26-30 8 2011. OP-02254.
- 10. Lee JH Kim GJ Choi BS et al.. Increasing late diagnosis in HIV infection in South Korea: 2000–2007. BMC Public Health 2010;10:411PMID: 20624319.ArticlePubMedPMC
- 11. UNAIDS.Global Report, UNAIDS Report on the Global AIDS Epidemic 2010.
- 12. Lee JH Hong KJ Wang JS et al.. Estimation of hospital-based HIV seroprevalence as a nationwide scale by novel method; 2002–2008 in Korea. BMC Public Health 2010;10:739PMID: 21114869.ArticlePubMedPMC
- 13. Detels R Jacobson L Margolick J et al. The multicenter AIDS Cohort Study, 1983 to ... Public Health 3;2012;126(3). 196−8. PMID: 22206985.ArticlePubMed
- 14. Bacon MC von Wyl V Alden C et al. The women’s interagency HIV study: an observational cohort brings clinical sciences to the bench. Clin Diagn Lab Immunol 9;2005;12(9). 1013−9. PMID: 16148165.ArticlePubMedPMC
- 15. Osih RB Taffe P Rickenbach M et al. Outcomes of patients on dual-boosted PI regimens: experience of the Swiss HIV Cohort Study. AIDS Res Hum Retroviruses 11;2010;26(11). 1239−46. PMID: 20929393.ArticlePubMedPMC
- 16. Dudley J Jin S Hoover D et al. The Multicenter AIDS Cohort Study: retention after 9§ years. Am J Epidemiol 8;1998;142(3). 323−30. PMID: 7631636.Article
- 17. CASCADE Collaboration.Concerted Action on Seroconversion to AIDS and Death in Europe. CASCADE; 1997.
Figure & Data
References
Citations
- Changing Patterns of HIV Epidemic in 30 Years in East Asia
S. Pilar Suguimoto, Teeranee Techasrivichien, Patou Masika Musumari, Christina El-saaidi, Bhekumusa Wellington Lukhele, Masako Ono-Kihara, Masahiro Kihara
Current HIV/AIDS Reports.2014; 11(2): 134. CrossRef - Can Stigma Still Distort the Spectrum of a Disease?
Hae-Wol Cho, Chaeshin Chu
Osong Public Health and Research Perspectives.2012; 3(2): 65. CrossRef
 PubReader
PubReader Cite
Cite
