Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 9(3); 2018 > Article
-
Original Article
Estimating the Incidence of Cases and Deaths Resulting from Hand, Foot and Mouth Disease and Its Related Socioeconomic Disease Burden in Republic of Korea (2010 – 2014) - Donghee Seo
-
Osong Public Health and Research Perspectives 2018;9(3):112-117.
DOI: https://doi.org/10.24171/j.phrp.2018.9.3.05
Published online: June 30, 2018
Division of Infectious Disease Surveillance, Korea Centers for Disease Control and Prevention, Cheongju, Korea
- *Corresponding author: Donghee Seo, Division of Infectious Disease Surveillance, Korea Centers for Disease Control and Prevention, Cheongju, Korea, Email: donnaseo@gmail.com
• Received: February 5, 2018 • Revised: May 13, 2018 • Accepted: June 10, 2018
Copyright ©2018, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
Abstract
-
Objectives
- Hand, Foot and Mouth disease (HFMD) is a highly contagious viral disease that affects young children and frequently causes epidemics. A vaccine is available in China (enterovirus 71) and, the Republic of Korea took the first step to develop a new vaccine. New vaccine development requires that disease burden is calculated in advance so the financial cost, morbidity and mortality can be measured.
-
Methods
- Data from National Sentinel Surveillance and health insurance systems of 1 million claimants were used. Direct medical and non-medical costs, indirect (caregiving and premature death) costs, cases and related deaths were summarized.
-
Results
- From 2010 to 2014, there were an estimated 3,605 to 9,271 cases of HFMD, with 1 to 3 deaths. The estimated socioeconomic disease burden ranged from 80.5 to 164.2 million USD and was similar to that of hepatitis A (93.6–103.8 million USD). Among each costs, costs of caregiving consisted of highest proportion mainly due to hiring caregivers (50% – 60%) or opportunity costs from day off (62% – 69%).
-
Conclusion
- Considering the social impact of HFMD, the estimated socioeconomic disease burden is not high and government policies need to focus on reducing the loss of work in caregivers.
- Hand Foot and Mouth disease (HFMD) is an acute viral infection caused by a variety of enteroviruses that affect young children (aged less than 10 years), especially children less than 5 years old [1]. Recently, there has been an increase in the number of children who go to daily childcare, and this seems to have an effect on shortening the cycle of major epidemics compared to previous years in Republic of Korea (ROK). Enteroviruses are highly contagious, so to prevent HFMD outbreaks and epidemics in ROK, new vaccination development is essential. However, the only HFMD vaccine (enterovirus 71) was developed and licensed for use only in China. A new HFMD vaccine needs to be developed and authorized for use in ROK.
- Government policies in ROK are in place to aid the development of a new HFMD vaccine so that it can be introduced into the national immunization program (NIP). However, introduction of a new vaccine program requires evaluation of cost-effectiveness. Therefore, the socioeconomic disease burden of HFMD in ROK needs to be estimated in advance.
Introduction
- 1. Study population
- Data from the national sentinel surveillance and national health insurance systems reported from 2010 to 2014 were used. The assumption was made that all patients visited outpatient clinics or were hospitalized.
- Due to limitations in access to all data, randomly sampled insurance data were used from 1 million people who claimed medical compensation from the national health insurance organization. To extract HFMD cases, patients were selected whose main diagnosis in insurance data terms were B08.4 or B08.5 within the KCD-10 code.
- 2. Estimating the incidence of cases and deaths resulting from hand, foot and mouth disease
- The estimation for number of HFMD cases and death in ROK was based on the annual occurrence rate of HFMD and was reverse calculated. We referred annual occurrence rates of HFMD from “KCDC Surveillance reports for infectious disease” from 2010 to 2014. Total number of patients who visited hospitals, especially the department of pediatrics were referred from the “Annual statistical reports of national health insurance system” from 2010 to 2014 [2].
- Estimated number of HFMD cases = total number of patients who visited department of pediatrics in a year × 100/annual occurrence rate of HFMD cases
- 3. Models for calculating economic disease burden of HFMD
- Since HFMD is an acute viral infectious disease and, disease progression and recovery occurs in a short period of time (less than 1 year), methodology was based on incidence rather than prevalence.
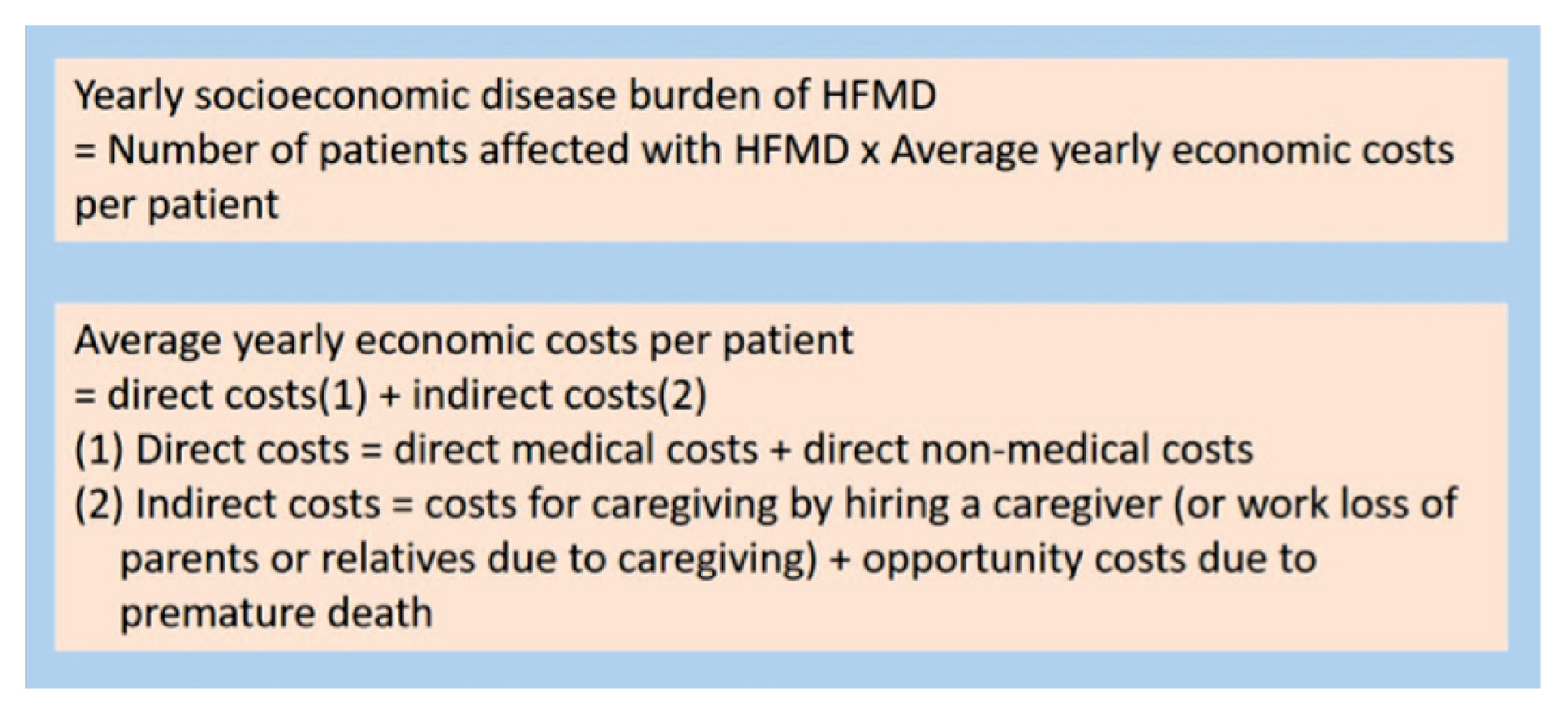
- Figure 1 shows the proposed formula for calculating economic costs due to HFMD [3]. Moreover, direct costs and indirect costs are considered, with several components which are described in Figure 2.
- From available data in the health insurance system, total medical costs for patients who visited outpatient clinics or who were hospitalized due to HFMD were used. The medical costs for prescribed medicines due to HFMD were calculated by multiplying annual total number of HFMD patients by the average number of prescribed days and average daily medical costs for the prescribed medicines.
- Medical costs for prescribed medicines = Annual total of HFMD patients × average number of prescribed days × average daily medical costs for the prescribed medicines
- For the estimation of direct non-medical costs, the in-depth report for Korea health panels was referred to assess the average daily transportation fee to and from hospital [4]. From the total number of patients selected (B08.4 or B08.5 within the KCD-10 insurance code) a random sample of patients were further selected. From 2010 to 2014, on average, only 4% of HFMD cases were admitted. Therefore, we used average values of transportation fees and hospital visits.
- Direct non-medical costs (transportation fee for visiting hospitals) = average daily transportation fee × average number of days for hospital visit × total number of HFMD patients in a year
- Costs for caregiving can be calculated in 2 ways according to the situation of the patients’ families. Most parents or family members could take care of a sick child, however, this may be impossible for other families in which case a caregiver is hired.
- Cost for caregiving (3) = average hourly salary of parents or relatives (or average hourly payment for hired caregiver) × 8 hours × average number of days for hospitalization (or outpatient clinic visits) × total number of HFMD cases in a year
- Opportunity costs due to premature deaths were calculated. Monthly numbers of HFMD cases were estimated by using the definition of proportion of HFMD cases. The proportion of HFMD cases was defined as the number of HFMD cases per thousand of cases who visited outpatient clinics. We estimated the number of premature deaths, adapting a case fatality rate of 0.03%, which is the lowest value among case fatality rates from reported outbreaks in the Western Pacific region considering a very low death rate in young children in ROK [5–9]. In the estimation the 5% discount rate was applied.
- We assumed that people could be employed for 36 years (if they did not die prematurely from HFMD) considering the average starting age of new recruits and the average retirement age listed in, “age employment status data in 2016 in ROK” [10]. Opportunity costs were estimated assuming complete hiring status for patients who had died prematurely from HFMD applying a 5% of discount rate. In addition, we used average values for starting and retirement age of work to make estimation simple. Therefore, all prematurely dead cases were regarded as being able to work for 36 years.
Materials and Methods
- In Table 1, the estimated number of HFMD cases and deaths in ROK between 2010 and 2014 are listed and show the number of HFMD cases was mainly influenced by epidemics. Estimated number of deaths due to HFMD ranged from 1 to 3, which seems rational considering the low death rates in young children in ROK. Cost due to premature deaths rose from 2.3 million to 7.2 million from 2010 to 2014.
- In 2008 and 2009, 5,870 and 6,338 HFMD cases were reported to the national surveillance system in ROK [11]. The number of HFMD cases was mainly influenced by whether there was a large epidemic or not in that year. However, the estimated numbers of HFMD cases between 2010 and 2014 seem to be similar to the figures in 2008 and 2009 [12]. Estimated number of deaths due to HFMD ranged from 1 to 3 which seemed reasonable considering the low death rates in young children in ROK. It is consistent with the fact that the cumulative number of deaths from HFMD was 9 until 2016.
- Table 2 shows referred values calculated for direct non-medical costs and indirect costs for transportation and caregiving. Estimated indirect costs of caregiving were calculated in 2 ways. By taking the average salary of caregivers and parents or relatives, based on gender, where a range of indirect costs were observed. In the case of caregiving by families, according to caregiver’s gender and contribution to the household income (e.g. 100% or 25%), indirect costs for caregiving resulted in different values. Where male caregivers contributed more, indirect costs for caregiving were higher due to gender differences in average salaries per hour.
- From 2010 to 2013, instead of average daily hospital visits or admitted period, the total number of hospital visits or annual admitted periods from health insurance data was adapted because it was not possible to obtain the exact number of total hospital visits or admitted period for 2014, so an estimated average daily hospital visits or admitted period per patient was used and multiplied by the total annual number of patients.
- In Table 3, socioeconomic disease burden of HFMD in ROK between 2010 and 2014 is shown. The economic costs had not increased annually since the total number of HFMD cases depended on whether there were more outbreaks, or a large epidemic in that year. Even though increased health insurance fees and inflation rates had an effect on economic costs, the differences in total number of HFMD cases offset the impact. The total individual patient costs during the period of infection with HFMD were significantly different between 2010 and 2014 as determined by ANOVA (p 0.021).
- The estimated total economic costs of HFMD in ROK between 2010 and 2014 ranged from 80.5 to 164.2 million USD. They were similar to the costs from hepatitis A infection which was previously treated as enterovirus infection and more than the costs from rotavirus infection. However, they were less than the socioeconomic burden of irritable bowel syndrome (Table 4). The 4 components (direct medical costs from outpatient clinics or hospitals, costs for the prescribed medicines, direct non-medical costs, cost for caregiving) consisting the socioeconomic burden of HFMD were revealed to be related to each other statistically by partial correlation analysis, after putting year as the control variable (Table 5).
Results
- In the Western Pacific region, widespread epidemics of HFMD have been reported in many countries including Australia, China, Japan and the ROK [13]. HFMD cases in ROK were mostly reported in summer and was similar to other Asian countries having comparable climates such as China and Japan [12].
- Therefore, during the peak period in summer, the incidence of complaints about sick children from parents and the media is heightened. HFMD seems to increase social concern after large epidemics that mostly affect young children, resulting in parents’ loss of work due to caregiving. In our model, we calculated the costs of caregiving adapting both ways of caregiving.
- Since caregivers hired by parents of sick children tend to be paid less than the average salary of parents, the costs for hiring caregivers were estimated to be lower. Previously hepatitis A virus was classified as an enterovirus, since it shared common characteristics. Therefore, the socioeconomic disease burden of HFMD was considered to be similar to that of hepatitis A virus. Most of the estimated socioeconomic disease burden of HFMD arises from the costs for caregiving. Therefore, the high socioeconomic concern for HFMD epidemics seems to be mainly due to the loss of labor and the resulting opportunity costs. There may be a need for new policies to make up for the labor loss, such as making it easier to hire caregivers by compensating the costs and providing systematic support for emergency, short-term hiring. Although we calculated the average increasing rate for socioeconomic disease burden of HFMD, the costs fluctuated yearly depending on the size and number of outbreaks. The budget for preparing and responding to national HFMD epidemics has to be changed to allow flexible responses according to the situation. In addition, 4 components that contribute to the socioeconomic burden of HFMD (direct medical costs from outpatient clinics or hospitals, costs for prescribed medicines, direct non-medical costs, and costs for caregiving), were revealed to be statistically related to each other, since they are all dependent on the number of HFMD cases in a year. In other words, if a new vaccine for HFMD was to be developed in the future, it may be a useful strategy to decrease these 4 components at the same time.
- Although the current study estimated socioeconomic disease burden of HFMD and compared it with those of other similar diseases such as rotavirus and hepatitis A virus infection, several assumptions were made and calculations were based on average values resulting in a less precise estimation.
Discussion
-
Acknowledgements
- Using data from sentinel surveillance and health insurance systems does not require IRB approval since they were all open to the public already and encrypted to inhibit recognizing personal information.
Acknowledgements
- 1. Zhao J, Jiang F, Zhong L, Sun J, Ding J. Age patterns and transmission characteristics of hand, foot and mouth disease in China. BMC Infect Dis 2016;16(1). 691PMID: 10.1186/s12879-016-2008-y. PMID: 27871252. PMID: 5117511.ArticlePubMedPMCPDF
- 2. NHI service. Annual statistical reports of national health insurance system. Annual statistical reports of national health insurance system. 2009–15.
- 3. Jung Y, Go S. The socioeconomic costs of diseases resulting in the top five causes of deaths. A book of the academy of finance in the Republic of Korea 2004;18(2). 77−102.
- 4. KIHASA. In-depth report for Korea health panels. 2010–2014.
- 5. Park S, Kim C, Go S. The socioeconomic costs due to smoking in 2007. Korean J Health Promot Dis Prev 2008;8(4). 219−27.
- 6. WPRO. WPRO Hand Foot and Mouth disease biweekly report. WPRO. 2010–2016.
- 7. Xing W, Liao Q, Viboud C, Zhang J, Sun J, Wu JT. Hand, foot, and mouth disease in China, 2008–12: an epidemiological study. Lancet Infect Dis 2014;14(4). 308−18. PMID: 10.1016/S1473-3099(13)70342-6. PMID: 24485991. PMID: 4035015.ArticlePubMedPMC
- 8. Khanh TH, Sabanathan S, Thanh TT, et al. Enterovirus 71-associated Hand, Foot, and Mouth Disease, Southern, Vietnam, 2011. Emerging Infect Dis 2012;18(12). 2002−5. PMID: 10.3201/eid1812.120929. PMID: 23194699. PMID: 3557876.ArticlePubMedPMC
- 9. Wang ZL, Xia AM, Li YF, et al. Socioeconomic burden of hand, foot and mouth disease in children in Shanghai, China. Epidemiol Infect 2016;144(1). 138−43. PMID: 10.1017/S0950268815001569.ArticlePubMed
- 10. KSIS. Age employment status. Korea statistical database. 2016.
- 11. KCDC. Surveillance report for infectious disease in 2009. Korea Center for Disease Control and Prevention; 2010.
- 12. KCDC. Surveillance report for infectious disease in 2016. Korea Center for Disease Control and Prevention; 2017.
- 13. WPRO. A Guide to clinical management and public health reponse for hand, foot and mouth disease (HFMD). WHO Library Cataloguing in Publication Data. 2011.
- 14. Yang BM, Jo DS, Kim YH, Hong JM, Kim JS. The Societal cost of rotavirus infection in South Korea. Korean J Pediatr 2008;51(9). 977−86. PMID: 10.3345/kjp.2008.51.9.977.Article
- 15. Kim K, Jeong BG, Ki M, et al. The costs of hepatitis A infections in South Korea. Epidemiol Health 2014;36:(e2014011).ArticlePDF
References
Figure 1Annual number of publications containing the term “biomarker” in the title which published from 1998 to 2017.
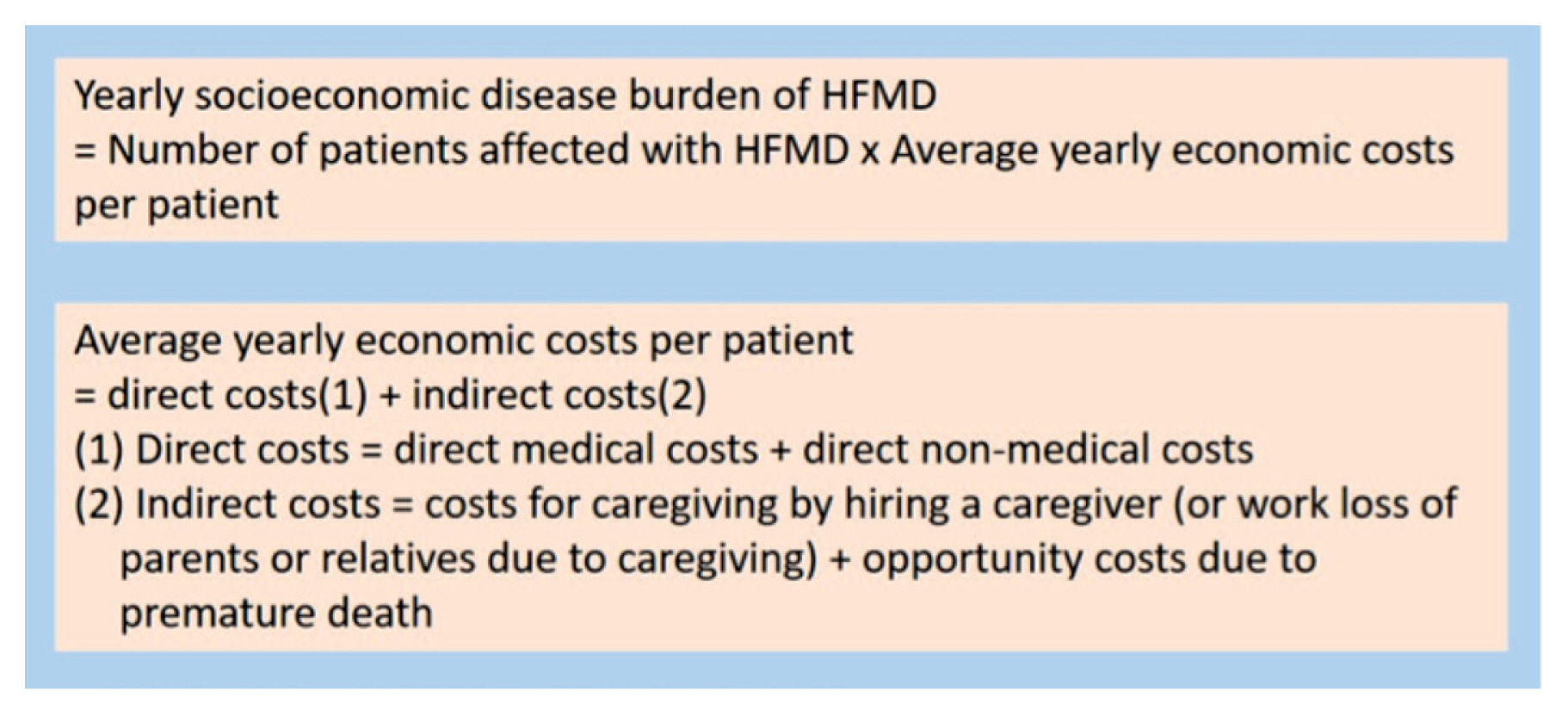
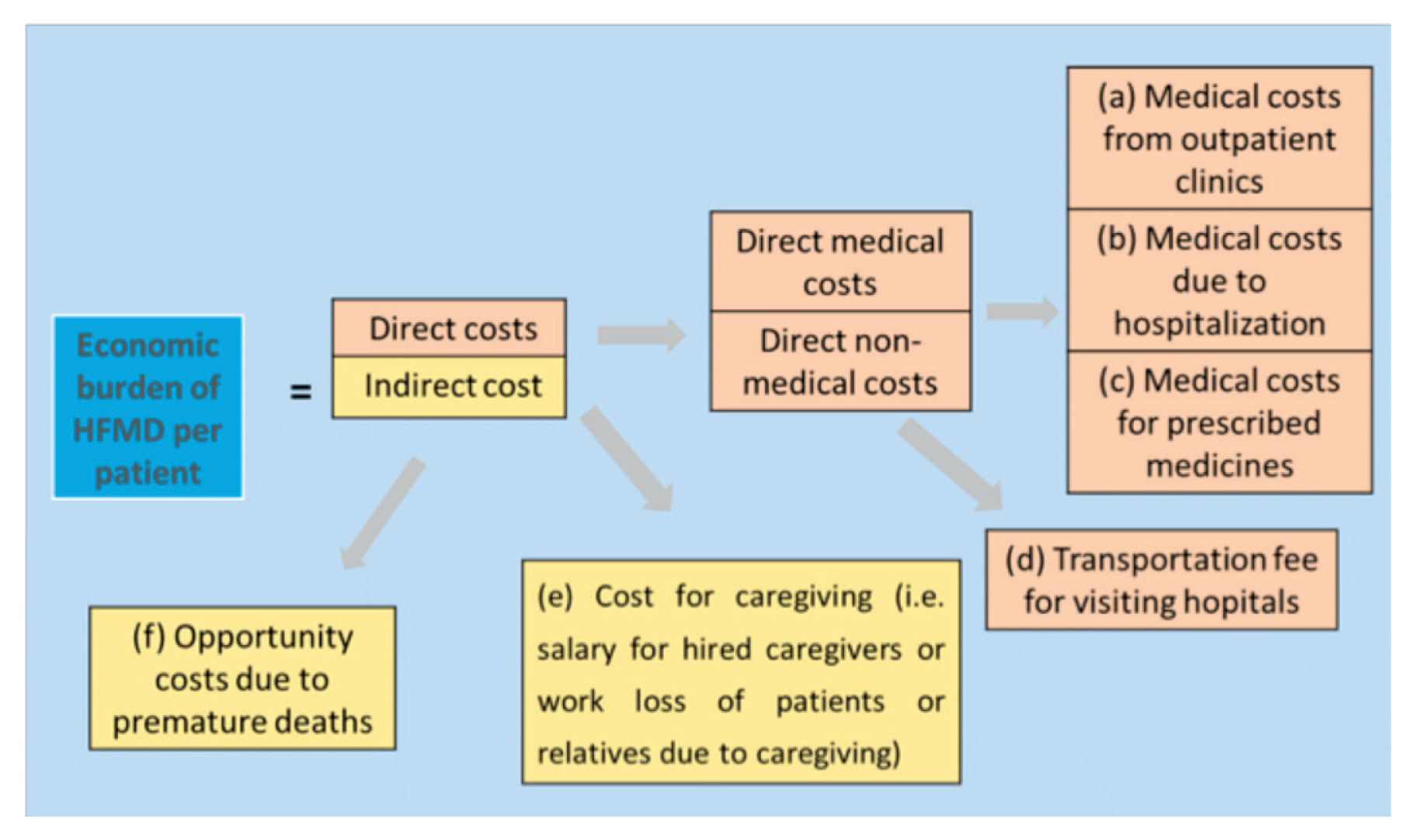
Table 1Estimated numbers of HFMD cases and deaths in ROK between 2010 and 2014.
| Estimated | 2010 | 2011 | 2012 | 2013 | 2014 |
|---|---|---|---|---|---|
| HFMD cases | 3,605 | 6,201 | 4,446 | 6,176 | 9,271 |
| Deaths | 1 | 2 | 1 | 2 | 3 |
| Costs due to premature deaths ($) | 2,340,326 | 4,229,498 | 3,243,290 | 4,651,594 | 7,248,965 |
Table 2Average daily transportation fee, average salary per hour and total and estimated hospital visits (admission period).
Table 3Economic burden of HFMD in ROK between 2010 and 2014.
Table 4Comparison of economic costs for four diseases (HFMD, Rotavirus, Hepatitis A, IBS).
| HFMD | Rotavirus | Hepatitis A | Irritable bowel syndrome | |
|---|---|---|---|---|
| Economic disease burden of the disease between 2010 and 2014 (million $) | 80.5~164.2 | 15.4~17.1 [14] | 93.6~103.8 [15] | 630.1~698.8 [15] |
Table 5The results of partial correlation tests among components consisting of the economic burden of HFMD.
Figure & Data
References
Citations
Citations to this article as recorded by 
- Association of public health and social measures on the hand-foot-mouth epidemic in South Korea
Sukhyun Ryu, Changhee Han, Sheikh Taslim Ali, Chiara Achangwa, Bingyi Yang, Sen Pei
Journal of Infection and Public Health.2023; 16(6): 859. CrossRef - Dynamical analysis for a reaction-diffusion HFMD model with nonsmooth saturation treatment function
Lei Shi, Hongyong Zhao, Daiyong Wu
Communications in Nonlinear Science and Numerical .2021; 95: 105593. CrossRef - A stage structure HFMD model with temperature-dependent latent period
Hongyong Zhao, Lei Shi, Jing Wang, Kai Wang
Applied Mathematical Modelling.2021; 93: 745. CrossRef - A reaction-diffusion HFMD model with nonsmooth treatment function
Lei Shi, Hongyong Zhao, Daiyong Wu
Advances in Difference Equations.2021;[Epub] CrossRef - Development and comparison of forecast models of hand-foot-mouth disease with meteorological factors
Tao Fu, Ting Chen, Zhen-Bin Dong, Shu-Ying Luo, Ziping Miao, Xiu-Ping Song, Ru-Ting Huang, Ji-Min Sun
Scientific Reports.2019;[Epub] CrossRef - Application of a combined model with seasonal autoregressive integrated moving average and support vector regression in forecasting hand-foot-mouth disease incidence in Wuhan, China
Jiao-Jiao Zou, Gao-Feng Jiang, Xiao-Xu Xie, Juan Huang, Xiao-Bing Yang
Medicine.2019; 98(6): e14195. CrossRef
 PubReader
PubReader Cite
Cite