Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 9(3); 2018 > Article
-
Short Communication
Case ofRickettsia typhi -induced Brain Abscess Mimicking Brain Tumor - Yoonhyuk Janga, Jangsup Moona, Jin-Sun Juna, Tae-joon Kima, Kyung-Il Parkb, Soon-Tae Leea, Keun-Hwa Junga, Sang Kun Leea, Kon Chua
-
Osong Public Health and Research Perspectives 2018;9(3):122-125.
DOI: https://doi.org/10.24171/j.phrp.2018.9.3.07
Published online: June 30, 2018
aDepartment of Neurology, Laboratory for Neurotherapeutics, Comprehensive Epilepsy Center, Center for Medical Innovations, Biomedical Research Institute, Seoul National University Hospital; Program in Neuroscience, Seoul National University College of Medicine, Seoul, Korea
bDepartment of Neurology, Seoul National University Hospital Healthcare System Gangnam Center, Seoul, Korea
- *Corresponding author: Kon Chu, Department of Neurology, Laboratory for Neurotherapeutics, Comprehensive Epilepsy Center, Center for Medical Innovations, Biomedical Research Institute, Seoul National University Hospital; Program in Neuroscience, Seoul National University College of Medicine, Seoul, Korea, E-mail: stemcell.snu@gmail.com
- † These two authors contributed equally to this work.
Copyright ©2018, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
Abstract
- Murine typhus is one of the most prevalent rickettsial infections in the world, caused by the bacterial genus Rickettsia. Though the disease manifests a relatively benign clinical course with fever, rash, and headache being the 3 classic symptoms, neurological complications may arise in patients that could become permanent. In this case study, a patient with a brain abscess caused by R typhi infection is described. Based upon the recent reemergence of arthropod-borne disease, the findings in this case are significant; R typhi can cause a brain abscess that mimics a brain tumor, which delays the diagnosis and appropriate management of the disease. Murine typhus should always be considered when performing the differential diagnosis of brain abscesses in South Korea.
- Murine typhus is one of the most prevalent rickettsial infections in the world, caused by Rickettsia bacteria [1] and transmitted by the rat flea, Xenopsylla cheopis, and causes problems for travelers who visit rural infected areas [2–4]. Though the disease manifests a relatively benign clinical course with the classic triad of fever, rash, and headache, the infection may lead to neurological complications in patients could be permanent [5].
- Compared to other rickettsial infections, R typhi invasion of the central nervous system is rare, but may result in a wide spectrum of severity, ranging from a mild headache to a life-altering coma [5, 6]. To date, all cases of infection with R typhi have been reported as meningitis and/or encephalitis associated with a severe systemic infection [5–7]. In this report, we describe a patient with R typhi infection that resulted in a brain abscess.
Introduction
- A 52 year old man was referred to the clinic with an intractable, ongoing (5 months), moderate headache in the vertex area. He was previously a fit and healthy individual who was working as a cook in a local restaurant in Seoul. After a vacation in August where he visited Gangwon-do (rural province of South Korea), he presented with a skin rash that covered his whole body. The rash lasted for 1 month and disappeared spontaneously without any treatment. He did not remember being bitten by an insect during the holidays, and as a precaution, he was denied contact with domestic or wild animals.
- In October, stabbing headaches recurred twice a day, accompanied by patient experiencing cold sensations and myalgia. There were no definite upper respiratory tract symptoms or gastrointestinal symptoms during the headache episodes.
- Although the patient had received supportive management for 2 months in a local clinic, the headaches persisted so he was referred to the Seoul National University Hospital, the following March.
- A physical examination did not reveal any abnormalities; his body temperature was 37.5°C, there was no skin rash, hepatomegaly, splenomegaly, or lymphadenopathy.
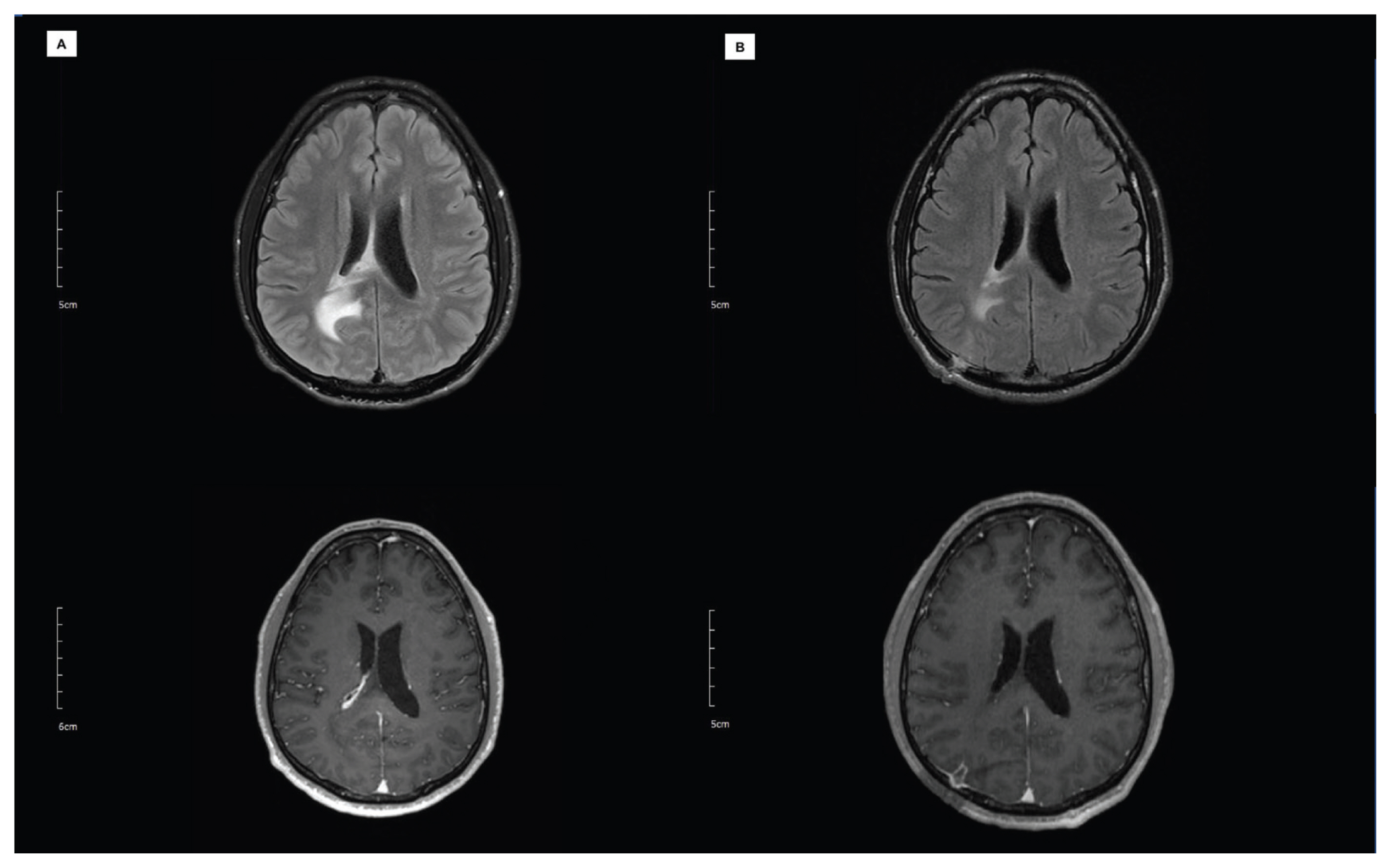
- The neurological examination was also normal, and laboratory findings were within the normal range showing white blood cell count of 9.93 × 103/μL and a C-reactive protein level of 0.32 mg/dL. The chest X-ray was normal. However, magnetic resonance imaging (MRI) of the brain disclosed a 2 cm mass near the right periventricular area (Figure 1A). With T1-weighted, gadolinium-enhanced imaging, the mass was observed along with the central cystic component. A cerebrospinal fluid (CSF) sample revealed a white cell count of 440/mL; 45% other cells, 42% lymphocytes, 13% polymorphonuclear cells, elevated proteins (107 mg/dL), and normal glucose (65 mg/dL, blood serum 121 mg/dL). In the serum and CSF, all cultures, viral polymerase chain reactions, and serological tests, including herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), varicella zoster virus, Epstein-Barr virus, cytomegalovirus, influenza, adenovirus, enterovirus, JC virus, measles, human immunodeficiency virus, human herpesvirus 6 (HHV-6) and human herpesvirus 8 (HHV-8), syphilis, Mycoplasma, Legionella, Mycobacterium, Chlamydia, Borrelia, Cryptococcus, Aspergillus, and Pneumocystis were all negative. Chest/abdominal computational tomography and echocardiography were also normal, disclosing no systemic infection source.
- The MRI scan and CSF sample did not indicate an infectious abscess but, to rule out a brain tumor, a stereotactic biopsy was performed. Aspiration of the lesion revealed a yellow fluid without foul odor that was negative for bacteria following culture. Whilst waiting for the pathology results, the patient received antibiotics according to a bacterial infection (ceftazidime 2g (3 times per day) + vancomycin 1g (2 times per day) + ampicillin/sulbactam 750mg (three times per day). After 5 days, pathology revealed a chronic, active inflammation with perivascular lymphoplasma cells and neutrophilic infiltration, without malignancy. Two more weeks of the empirical antibiotics were maintained. The patient’s headaches did not subside and a follow-up MRI did not show a full response (Figure 1B) to antibiotic treatment. Thus, additional serum tests were requested from the Korea Centers for Disease Control and Prevention (KCDC; Cheongju-si, South Korea) to test for atypical bacteria: Rickettsia spp., Leptospira spp., and Brucella. Ceftazidime and ampicillin/sulbactam were administered for an additional 2 weeks until the result of a serum immunofluorescence assay was received. Antibodies against R typhi to a titer of IgM 1:32 and IgG 1:64 were detected. According to the diagnostic criteria of murine typhus, 1 of the following is required: 1) an IgM titer of ≥ 1:32, 2) a single IgG antibody titer of ≥ 1:128, or 3) a 4-fold increase in sera antibody titers between the acute phase and the convalescent phase [8].
- Therefore, the patient’s lesion was diagnosed as a brain abscess caused by R typhi Ceftazidime and ampicillin/sulbactam were maintained for an additional 2 weeks without changing to doxycycline dosing, because the patient responded to the combination during the 4th week of treatment. His headaches disappeared completely after a total of 6 weeks of antibiotic treatment.
Case Report
- Rickettsial infection evokes a pathogenic process of endothelial cell invasion with destruction of integrity and increased permeability of the endothelium, leading to the term ‘Rickettsial vasculitis’ [9]. Rickettsial vasculitis of the vascular endothelium can lead to various clinical symptoms: maculopapular rash, interstitial pneumonia, acute renal failure, and meningoencephalitis [5, 10, 11].
- Theoretically, the choroid plexus can be a target of rickettsial vasculitis because it consists of a network of capillary endothelial cells. However, the abscess formation via the choroid plexus caused by Rickettsia spp. is extremely rare, and this report is thought to be the first to describe an R typhi infection that caused a brain abscess in a human patient. The MRI revealed the T1-enhanced mass along the right lateral ventricle, confirmed as a pyogenic abscess by aspirational biopsy. The lesion was potentially the origin of the patient’s mild, recurrent headache that was accompanied by a sensation of cold and myalgia. This finding is supported by the result of the immunofluorescence assay, which showed a high IgM titer, even though the test was performed 5 months after the onset of symptoms.
- Rickettsial infection was not suspected initially, not only due to its rarity but also because the patient showed a relatively mild, chronic course of clinical manifestations. Unlike a typical bacterial infection of the central nervous system, the lesion did not induce a high fever or altered mental state. Thorough work-up with laboratory tests, whole-body computational tomography, and echocardiography confirmed that there was no other systemic involvement. Moreover, the bacterial culture studies were all negative. Therefore, a brain tumor was considered a more likely diagnosis than a brain abscess.
- The current study has limitations; the diagnostic criteria for antibody titers were incomplete because 2 consecutive samples were not tested so even if the IgM antibody titer of the patient’s serum was greater than 1:32 and the IgG antibody titer was as low as 1:64 this result was not validated with a comparative results from additional samples. However, the low IgG antibody titer could be confirmed because 3 weeks earlier empirical antibiotics were administered for cryptogenic brain abscess. Another consideration is that the immunofluorescence assay uses an indirect method of detecting host responses, so despite this method being the gold standard of murine typhus diagnosis (sensitivity 53–85%, specificity 99%) this introduces a limitation to the study [12]. Therefore, the fact that diagnosis of R typhi was supported by the other comprehensive tests rules out other etiologies, and the clinical course of the patient showed the classic triad of murine typhus. Doxycyclin, which is the treatment of choice for Rickettsia infection [4], may have alleviated the patient’s symptoms more quickly had the diagnosis not been delayed. However, it is meaningful that the combination of ceftazidime and ampicillin/sulbactam, which is the alternative treatment for cryptogenic brain abscess [13], resolved the patient’s symptoms.
- Since the first report of a patient with murine typhus in 1959 in South Korea, the annual number of patients with murine typhus increased to 87 in 2008. The incidence of the disease seemed to be on the decline, but in 2014, 20 cases were reported and an increased trend has been reported by KCDC [14]. Based upon the recent reemergence of arthropod-borne disease, this case is remarkable; R typhi can cause a brain abscess to mimic a brain tumor. This delays the diagnosis and appropriate management of the disease. It is difficult to differentiate between a brain abscess and a brain tumor because both appear similarly on an MRI and both commonly cause seizures in the patient. Thus, murine typhus should always be considered in the diagnosis of brain abscess in South Korea.
Discussion
-
Conflicts of Interest
The authors declare no competing financial interests.
-
Ethical Publication Statement
We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Article information
- 1. Raoult D, Roux V. Rickettsioses as paradigms of new or emerging infectious diseases. Clin Microbiol Rev 1997;10(4). 694−719. PMID: 9336669. PMID: 172941.ArticlePubMedPMC
- 2. Walter G, Botelho-Nevers E, Socolovschi C, Raoult D, Parola P. Murine Typhus in Returned Travelers: A Report of Thirty-Two Cases. Am J Trop Med Hyg 2012;86(6). 1049−53. PMID: 10.4269/ajtmh.2012.11-0794. PMID: 22665617. PMID: 3366521.ArticlePubMedPMC
- 3. Jensenius M, Fournier P-EE, Raoult D. Rickettsioses and the international traveler. Clin Infect Dis 2004;15 39(10). 1493−9. PMID: 10.1086/425365. PMID: 15546086.ArticlePubMedPDF
- 4. Civen R, Ngo V. Murine typhus: an unrecognized suburban vectorborne disease. Clin Infect Dis 2008;46(6). 913−8. PMID: 10.1086/527443. PMID: 18260783.ArticlePubMedPDF
- 5. Masalha R, Merkin-Zaborsky H, Matar M, Zirkin HJ, Wirguin I, Herishanu YO. Murine typhus presenting as subacute meningoencephalitis. J Neurol 1998;245(10). 665−8. PMID: 10.1007/s004150050264. PMID: 9776466.ArticlePubMedPDF
- 6. Vallejo-Maroto I, García-Morillo S, Wittel MB, et al. Aseptic meningitis as a delayed neurologic complication of murine typhus. Clin Microbiol Infect 2002;8(12). 826−7. PMID: 10.1046/j.1469-0691.2002.00502.x.ArticlePubMed
- 7. Moy W, Ooi S. Abducens Nerve Palsy and Meningitis by Rickettsia typhi. Am J Trop Med Hyg 2015;92(3). 620−4. PMID: 10.4269/ajtmh.14-0559. PMID: 4350562.ArticlePubMedPMC
- 8. Scola LA, Raoult D. Laboratory Diagnosis of Rickettsioses: Current Approaches to Diagnosis of Old and New Rickettsial Diseases. J Clin Microbiol 1997;35(11). 2715−27. PMID: 9350721. PMID: 230049.ArticlePubMedPMC
- 9. Walker DH, Ismail N. Emerging and re-emerging rickettsioses: endothelial cell infection and early disease events. Nat Rev Microbiol 2008;6(5). 375−86. PMID: 18414502.ArticlePubMedPDF
- 10. Schulze MH, Keller C, Müller A, et al. Rickettsia typhi Infection with Interstitial Pneumonia in a Traveler Treated with Moxifloxacin. J Clin Microbiol 2011;49(2). 741−3. PMID: 10.1128/JCM.01201-10. PMID: 3043471.ArticlePubMedPMC
- 11. Hernández Cabrera M, Angel-Moreno A, Santana E, et al. Murine typhus with renal involvement in Canary Islands, Spain. Emerg Infect Dis 2004;10(4). 740−3. PMID: 10.3201/eid1004.030532. PMID: 15200874. PMID: 3323099.ArticlePubMedPMC
- 12. Paris DH, Dumler SJ. State of the art of diagnosis of rickettsial diseases: the use of blood specimens for diagnosis of scrub typhus, spotted fever group rickettsiosis, and murine typhus. Curr Opin Infect Dis 2016;29(5). 433−9. PMID: 10.1097/QCO.0000000000000298. PMID: 27429138. PMID: 5029442.ArticlePubMedPMC
- 13. Arlotti M, Grossi P, Pea F, et al. Consensus document on controversial issues for the treatment of infections of the central nervous system: bacterial brain abscesses. Int J Infect Dis 2010;14( Suppl 4). S79−92. PMID: 10.1016/j.ijid.2010.05.010. PMID: 20846891.ArticlePubMed
- 14. KCDC. 2016 Infectious diseases surveillance yearbook. Osong: KCDC; 2016.
References

Figure & Data
References
Citations
- Meningoencephalitis and retinal vasculitis due to rickettsial infection
Louisa Lehner, Stephan Thurau, Konstantin Pusl, Steffen Tiedt, Florian Schöberl, Robert Forbrig, Günter Höglinger, Michael Strupp
Journal of Neurology.2024; 271(3): 1469. CrossRef - Giant Actinomyces brain abscess in an immunocompetent child: A management strategy
Nicole H. Chicoine, Jackson Griffith-Linsley, Joling Goh, John J. Manaloor, Jeffrey S. Raskin
Surgical Neurology International.2021; 12: 325. CrossRef
 PubReader
PubReader Cite
Cite