
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 8(1); 2017 > Article
-
Original Article
Knowledge Management Enablers and Process in Hospital Organizations - Hyun-Sook Lee
-
Osong Public Health and Research Perspectives 2017;8(1):26-33.
DOI: https://doi.org/10.24171/j.phrp.2017.8.1.04
Published online: February 28, 2017
Department of Health Administration, Kongju National University, Kongju, Korea
- Corresponding author: Hyun-Sook Lee, E-mail: lhs@kongju.ac.kr
Copyright © 2017 Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
-
Objectives
- This research aimed to investigate the effects of knowledge management enablers, such as organizational structure, leadership, learning, information technology systems, trust, and collaboration, on the knowledge management process of creation, storage, sharing, and application.
-
Methods
- Using data from self-administered questionnaires in four Korean tertiary hospitals, this survey investigated the main organizational factors affecting the knowledge management process in these organizations. A total of 779 questionnaires were analyzed using SPSS 18.0 and AMOS 18.0.
-
Results
- The results showed that organizational factors affect the knowledge management process differently in each hospital organization.
-
Conclusion
- From a managerial perspective, the implications of these factors for developing organizational strategies that encourage and foster the knowledge management process are discussed.
- Knowledge management (KM) has been recognized as being central to product and process innovation, executive decision making, and organizational adaptation and renewal [1]. To achieve competitive sustainability, many organizations are launching extensive KM efforts [2]. Several KM enablers have been recognized in previous research and many of these factors overlap [3–5]. In this research, KM enablers are categorized into six categories such as organization structure, leadership, information technology (IT) systems, learning, trust, and collaboration. KM starts with the process of knowledge creation, knowledge storage, knowledge sharing, and knowledge application among employees to support the organization becoming more competitive. Several studies have demonstrated that the KM process is essential because it enables organizations to enhance innovation performance and reduce redundant learning efforts [6,7]. Moreover, when individual members share their knowledge or expertise, it is crucial for organizations to increase significant organizational resources and decrease time wasted in trial-and error [8]. However, the lack of a KM process has proven to be one of the major barriers to effective KM [9]. The success of an organization ultimately depends on the KM process, which creates long-term benefits, learns new techniques, solves problems, creates core competencies, and adapts to new situations [10].
- Hospital organizations are knowledge-intensive environment involving rapidly changing medical technologies, and requiring tools, skills, and methods with more knowledge resources. Hospital organizations have been interested in communities of practice as a means of transferring and generating knowledge within them [11–14]. However, unlike other organizations, hospital organizations reveal one of the most complex structures in our society. They require a highly divergent set of activities, such as providing health care, testing, diagnosis, and treatment and planning and executing hospitalization, surgical interventions, and other procedures, as well as understanding complicated decision-making processes and networks. Due to the organizational culture and systems within hospital organizations, setting up successful KM has not been easy. Different departments within them must adopt the KM process to share employees’ new knowledge and various techniques in a number of ways [15]. Various studies have focused on the relationship between KM enablers and processes [16–18]. However, studies in the health-care field concerning how KM enablers affect the KM process remain rare. The KM process rests in the brain of the person who has this particular knowledge [19]. Therefore, hospital organizations need to understand organizational structure, culture, and systems to perform successful KM.
- Concepts derived from a literature review of KM, its enabling factors, and the KM process have been presented in this section. The next section describes the research model and then reviews data collection and data analysis. The subsequent section presents the results of this study. The last section is a discussion of this study’s findings and the conclusions of this research.
INTRODUCTION
- 1. Hypotheses and research model
- This research hypothesizes that the four modes of the KM process are subject to several organizational forces by hospital organizations and their management. Based on the previous literature review, we proposed that organizational structure, leadership, IT systems, learning, trust, and collaboration affect the KM process, and we aimed to assess their influence in four different hospitals. The following research model is derived from the previous discussion on the influence of KM enablers on the KM process (Figure 1).
- This study did not propose definite hypotheses about which constructs positively or negatively affect KM processes, but rather it aimed to compare the importance of these organizational forces for each hospital.
- 2. Sample and data collection
- The main criteria for selecting the subjects were that they must be knowledge workers involved in some knowledge tasks in their hospital organizations. Because hospitals mainly focus on medical and administrative areas, it is difficult to identify KM enablers and the KM process questions. Therefore, this survey only focused on large-sized hospitals that have a vision and a mission about hospital management, medical care, research and development, education, hospital culture and systems, and their employees’ minds including “Medical Innovation” and “Administration Innovation” strategies. There are 43 tertiary hospitals in Korea. From these 43 tertiary hospitals, a sample of 779 employees including nursing specialists, clinical technicians, and administrative staff were randomly selected from 4 tertiary hospitals in Seoul and Gyeonggi-do. All the participants voluntarily took part in this research and were also diverse in terms of gender and position (Table 1). The current study contributes to KM research by further clarifying which KM enablers are essential for the KM process to occur effectively. The survey that is analyzed in this paper is part of an effort to measure the success of this initiative.
- To measure the variables, this study used a multiple-item scale derived from existing studies. The quantitative analysis is drawn from a 69-item questionnaire using a 7-point Likert scale (ranging from 1 = strongly disagree to 7 = strongly agree). The questionnaire items were set up to inhibit insincere answers and then normalized. Scores closer to 7 were interpreted as positive, while scores closer to 1 were negative. The questionnaire itself was developed over many years with the collaboration of KM researchers from several universities in Korea.
- The total number of respondents for the targeted hospitals was 779, with hospital A accounting for 26.3% (205), hospital B 24.5% (191), hospital C 24.0% (187), and hospital D 25.2% (196) of respondents.
- 3. Measures
- To select relevant constructs, this study adopted an exploratory approach in which several factor analyses were conducted with KM enablers and KM process factors. The independent constructs were related to KM enablers including organizational structure, leadership, IT systems, learning, trust, and, collaboration. The dependent constructs related to the KM process were creation, storage, sharing, and application of knowledge. These constructs have already been subjected to factor analysis [9], and are consistent with the theoretical basis of this work.
- This survey presents the results of reliability and validity tests. An analysis was performed on the 30 items that measured the components of KM enablers and KM processes. Cronbach’s alpha was used to examine the reliability of the instruments. Alpha values over 0.6 are generally considered acceptable. All constructs had alpha values higher than 0.6, ranging from 0.607 to 0.917. Factor analysis with varimax rotation was used to check the discriminant validity of the constructs. Factor analysis of the KM enablers and the KM process is shown in Table 2. The relatively high values for reliability and validity imply that the instruments used in this study were adequate.
- 4. Descriptive statistics
- Table 3 reveals the results of employees’ responses about KM activities in their hospitals. All four hospitals believed that major knowledge resides in the individual brain, groupware, and personal computers. Many respondents of hospital A (60.0%), hospital B (66.0%), hospital C (58.3%), and hospital D (52.6%) thought that their knowledge exists in individual brains. Barriers to KM in all four hospitals are the lack of enthusiasm for learning, the absence of collaborative culture, and lack of time. Most respondents of hospital A (75.6%), hospital B (75.9%), hospital C (84.5%), and hospital D (71.9%) agreed that one of the barriers to KM is the lack of enthusiasm for learning. Ways to inspire KM in hospitals are clear vision and consistent impulse, the link between hospital work processes and KM, professional workforce and budget allocation, fair rewards, and so on. Many respondents of hospital A (48.8%), hospital B (48.7%), hospital C (50.3%), and hospital D (51.5%) thought that the most important ways to inspire KM are clear vision and consistent impulse.
MATERIALS AND METHODS
- Multiple regression analyses were examined for each hospital sample with the six KM enablers. The independent variables were organizational structure, leadership, IT systems, learning, truth, and collaboration, while the dependent variables were application, storage, sharing, and application of knowledge. The research model was evaluated based on the amount of variance in the dependent constructs accounted for by the model (R2). For each hypothesis, models were run for each of the dependent variables separately as shown in Tables 4–7. The absolute value of the beta coefficient indicates which of the KM enablers have a greater impact on the KM process in each multiple regression analysis.
- In the hospital A sample (valid n = 205), the research model explained 18% of the variance for knowledge creation, 13% for knowledge storage, 29% for knowledge sharing, and 24% for knowledge application (p < 0.001). IT systems show the strongest effect on knowledge application (p < 0.001), and truth on knowledge creation and knowledge sharing (p <0.05), while leadership correlated with knowledge sharing (p < 0.05) (Table 4).
- In the hospital B sample (valid n = 191), the research model explained 15% of the variance for knowledge creation (p < 0.001), 11% for knowledge storage, 10% for knowledge sharing, and 9.8% for knowledge application (p < 0.01 or p < 0.001). Collaboration explains the most significant variance in all four KM processes that affect knowledge creation (p < 0.001), knowledge sharing, knowledge application, and knowledge storage (p < 0.05). IT systems showed the strongest effect on knowledge storage (p < 0.01), while leadership equally affected knowledge creation and knowledge storage (p < 0.05) (Table 5).
- In the hospital C sample (valid n = 187), the research model explained 16% of the variance for knowledge creation, 22% for knowledge storage, 16% for knowledge sharing, and 13% for knowledge application (p < 0.001). IT systems showed the strongest effect on knowledge creation and knowledge application (p < 0.05) and collaboration on knowledge sharing and knowledge application (p < 0.05) (Table 6).
- In the hospital D sample (valid n = 196), the research model explained 38% of the variance for knowledge creation, 29% for knowledge storage, 39% for knowledge sharing, and 43% for knowledge application (p < 0.001). Both leadership and IT systems explained the most significant variance in all four KM processes. Leadership showed the strongest effect on knowledge creation (p < 0.05), knowledge storage (p < 0.01), knowledge sharing (p < 0.05), and knowledge application (p < 0.05), IT systems showed significant effects on knowledge creation (p < 0.05), knowledge storage (p < 0.01), knowledge sharing (p < 0.05), and knowledge application (p < 0.01), while truth correlated with knowledge storage (p < 0.01), knowledge sharing (p < 0.001), and knowledge application (p < 0.0) (Table 7).
- Table 8 summarizes the findings of the multiple regression analyses assessing the effects of organizational structure, leadership, IT systems, learning, truth, collaboration on each KM process for the of samples A, B, C, and D hospitals.
RESULTS
- There is heightened awareness of the importance of KM in the healthcare field, especially for hospital organizations. However, KM is still a complex knowledge area with much more to be explored [20]. This is reflected in the results of the statistical analysis of the survey data, with the hospital samples being much more significant in the KM process as defined by Alavi and Leidner’s model [9].
- The regression model of hospital A, although significant, provided the lowest explanatory power among the four hospitals, and revealed that truth affects both knowledge creation and knowledge sharing, that leadership contributes to knowledge sharing, and that IT systems strongly influence knowledge application (Table 3). However, not all organizational factors affect knowledge storage (Table 3). Regarding all factors, the hospital A sample showed the factors related to KM processes, truth, leadership, and IT systems. Leaders will foster values like trust that are necessary for knowledge sharing to flourish [21,22]. When trust is high, individuals are more prone to participate in knowledge sharing, resulting in knowledge creation gain [23]. To achieve creation of new knowledge for the hospital, organizational knowledge must be shared and applied through trust with members.
- In terms of the regression analysis of hospital B shown in Table 4, the most striking result for the hospital B sample is the impact that collaboration has on all KM processes of knowledge creation, knowledge storage, knowledge sharing, and application, while leadership correlated with knowledge creation and knowledge sharing. Compared to hospitals A and C, the second remarkable result for the hospital B sample was the impact that leadership, IT systems, truth, and collaboration had on knowledge storage. These findings suggest that collaborative culture affects knowledge creation through increasing knowledge exchange [24] and high collaboration helps the KM process to set mutual purposes for performance [25]. According to Davenport and Prusak [19], top managers advocate that the behaviors of knowledge sharing within an organization become possible when knowledge sharing is considered as a fundamental resource for creating value.
- The regression model of hospital C, although significant, provided lower explanatory power than hospitals A and B, and revealed that IT systems affect both knowledge creation and knowledge application, that collaboration contributes to both knowledge sharing and knowledge application, and that leadership influences knowledge sharing. Similar to hospital A, not all organizational factors affect knowledge storage (Table 3). These three organizational factors—IT systems, leadership, and collaboration—are consistent with working together characterized by strong leadership. These findings suggest that, information and communication technology can enable rapid search, access, and retrieval of information, and can support communication and collaboration among employees [26].
- In terms of the regression analysis of Hospital D shown in Table 4, the four KM processes were most correlated with the impact of leadership and IT systems that promote knowledge application, storage, and sharing [27], while truth affects knowledge storage, knowledge sharing, and knowledge application. Eventually, the top managers’ support as an essential requirement for the successful KM establishes organizational culture to share employees’ knowledge within the organization [28]. The top managers of hospitals must try to support an important role of providing organizational culture and systems to create and share employees’ knowledge based on truth.
- This analysis reveals that deliberate and continued practice of KM, as demonstrated in the tertiary hospitals in Korea, reflects employees’ opinions about the KM activities of hospitals. Most workers in the four hospitals believed that major knowledge resides in individual brains, groupware, and personal computers. Many respondents thought that barriers to KM were the lack of enthusiasm for learning, the absence of collaborative culture, and lack of time. All of them thought that the most important way to inspire KM involved clear vision and consistent impulse. Therefore, there is a strong need for systematic management such as clear vision, budget allocation, fair rewards, task forces team, and the link between hospital work processes and the activities of KM.
- Additionally, this study presented the main factors, variables, and links between KM enablers and the KM process among these hospitals. Each hospital displayed very different patterns of KM and organizational features. The regression model showed that different organizational factors—especially IT systems, truth, and collaboration—were responsible for the resulting KM profiles of each hospital: truth in hospital A, collaboration in hospital B, and IT systems in both hospitals C and D.
- Although these findings are specific to the hospitals surveyed here, they can be considered for the development of practical strategies to enhance an understanding of critical factors between KM enablers and KM processes. Knowledge managers of each hospital must build an organization culture and systems and continuously educate employees about KM based on trust and collaboration.
DISCUSSION
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
Article information
- 1. Earl M. Knowledge management strategies: toward a taxonomy. J Manag Inf Syst 2001;18:215−33.Article
- 2. Gold AH, Malhotra A, Segars AH. Knowledge management: an organizational capabilities perspective. J Manag Inf Syst 2001;18:185−214.Article
- 3. Von Krogh G, Ichijo K, Nonaka I. Enabling knowledge creation: how to unlock the mystery of tacit knowledge and release the power of innovation. New York: Oxford University Press; 2000. PMID: 10.1007/978-1-349-62753-0.
- 4. Malhotra A, Majchrzak A. Enabling knowledge creation in farflung teams: best practices for it support and knowledge sharing. J Knowl Manag 2004;8:75−88. https://doi.org/10.1108/13673270410548496. PMID: 10.1108/13673270410548496.Article
- 5. Baskerville R, DulipovicI A. The theoretical foundations of knowledge management. Knowl Manag Res Pract 2006;4:83−105. https://doi.org/10.1057/palgrave.kmrp.8500090. PMID: 10.1057/palgrave.kmrp.8500090.Article
- 6. Calantone RJ, Cavusgil ST, Zhao Y. Learning orientation, firm innovation capability, and firm performance. Ind Mark Manag 2002;31:515−24. https://doi.org/10.1016/S0019-8501(01)00203-6. PMID: 10.1016/S0019-8501(01)00203-6.Article
- 7. Scarbrough H. Knowledge management, HRM and innovation process. Int J Manpow 2003;24:501−16. https://doi.org/10.1108/01437720310491053. PMID: 10.1108/01437720310491053.Article
- 8. Lin CP. To share or not to share: modeling knowledge sharing using exchange ideology as a moderator. Pers Rev 2007;36:457−75. https://doi.org/10.1108/00483480710731374. PMID: 10.1108/00483480710731374.Article
- 9. Alavi M, Leidner DE. Review: knowledge management and knowledge management systems: conceptual foundations and research issues. MIS Quarterly 2001;25:107−46. https://doi.org/10.2307/3250961. PMID: 10.2307/3250961.Article
- 10. Liao S, Fei WC, Chen CC. Knowledge sharing, absorptive capacity, and innovation capability: an empirical study of Taiwan’s knowledge-intensive industries. J Inf Sci 2007;33:340−59. https://doi.org/10.1177/0165551506070739. PMID: 10.1177/0165551506070739.Article
- 11. Currie G, Finn R, Martin G. Spanning boundaries in pursuit of effective knowledge sharing within networks in the NHS. J Health Organ Manag 2007;21:406−17. https://doi.org/10.1108/14777260710778934. PMID: 10.1108/14777260710778934. PMID: 17933372.ArticlePubMed
- 12. Caldwell BS. Knowledge sharing and expertise coordination of event response in organizations. Appl Ergon 2008;39:427−38. https://doi.org/10.1016/j.apergo.2008.02.010. PMID: 10.1016/j.apergo.2008.02.010. PMID: 18384752.ArticlePubMed
- 13. Rangachari P. Knowledge sharing networks related to hospital quality measurement and reporting. Health Care Manage Rev 2008;33:253−63. https://doi.org/10.1097/01.HMR.0000324910.26896.91. PMID: 10.1097/01.HMR.0000324910.26896.91. PMID: 18580305.ArticlePubMed
- 14. Graham JM, Brinson M, Magtibay LV, et al. Virtual patient safety rounds: one hospital system’s approach to sharing knowledge. J Healthc Qual 2009;31:48−52. https://doi.org/10.1111/j.1945-1474.2009.00047.x. PMID: 10.1111/j.1945-1474.2009.00047.x. PMID: 19813561.ArticlePubMed
- 15. Shnhoras EM. Culture in hospital organizations and cultural policies for coordinating communication and learning. Elect J Commun Inf Innov Health 2007;1:45−55. https://doi.org/10.3395/reciis.v1i1.45en.Article
- 16. van Den Hooff B, de Ridder JA. Knowledge sharing in context: the influence of organizational committment, communication climate and CMC cse on knowledge sharing. J Knowl Manag 2004;8:117−30. https://doi.org/10.1108/13673270410567675. PMID: 10.1108/13673270410567675.Article
- 17. Bock GW, Zmud RW, Kim YG, et al. Behavioral intention formation in knowledge sharing: examining the roles of extrinsic motivators, social-psychological forces, and organizational climate. MIS Quarterly 2005;29:87−111.Article
- 18. Yeh YJ, Lai SQ, Ho CT. Knowledge management enablers: a case study. Ind Manag Data Syst 2006;106:793−810. https://doi.org/10.1108/02635570610671489. PMID: 10.1108/02635570610671489.Article
- 19. Davenport TH, Prusak L. Working knowledge: how organizations manage what they know. Boston, MA: Harvard Business School Press; 1998.
- 20. Castillo LAM, Cazarini EW. Integrated model for implementation and development of knowledge management. Knowl Manag Res Pract 2014;12:145−60. https://doi.org/10.1057/kmrp.2012.49. PMID: 10.1057/kmrp.2012.49.Article
- 21. Light Z, Craig C, Hanifa S. The trust factor: Design team knowledge sharing culture. Proceedings of the World Congress on Engineering 2013;3:1−6. Available from: http://www.iaeng.org/publication/WCE2013/WCE2013_pp1583-1588.pdf.
- 22. Holste JS, Fields D. Trust and tacit knowledge sharing and use. J Knowl Manag 2010;14:128−40. https://doi.org/10.1108/13673271011015615. PMID: 10.1108/13673271011015615.Article
- 23. Saeed T, Tayyab B, Anis-Ul-Haque M, et al. Knowledge management practices: role of organisation culture. Proc ASBBS 2010;17:1027−36.
- 24. Nahapiet J, Ghoshal S. Social capital, intellectual capital, and the organizational advantage. Acad Manag Rev 1998;23:242−66. https://doi.org/10.2307/259373.Article
- 25. Kirkman BL, Tesluk PE, Rosen B. The impact of demographic heterogeneity and team leader-team member demographic fit on team empowerment and effectiveness. Group Organ Manag 2004;29:334−68. https://doi.org/10.1177/1059601103257412. PMID: 10.1177/1059601103257412.Article
- 26. Huysman M, Vulf V. IT to support knowledge sharing in communities, towards a social capital analysis. J Inf Technol 2006;21:40−51. https://doi.org/10.1057/palgrave.jit.2000053. PMID: 10.1057/palgrave.jit.2000053.Article
- 27. Ndlela LT, du Toit ASA. Establishing a knowledge management programme for competitive advantage in an enterprise. Int J Inf Manag 2001;21:151−65. https://doi.org/10.1016/S0268-4012(01)00007-X. PMID: 10.1016/S0268-4012(01)00007-X.Article
- 28. Alavi M, Kayworth TR, Leidner DE. An empirical examination of the influence of organizational culture on knowledge management practices. J Manag Inf Syst 2006;22:191−224. https://doi.org/10.2753/MIS0742-1222220307. PMID: 10.2753/MIS0742-1222220307.Article
REFERENCES
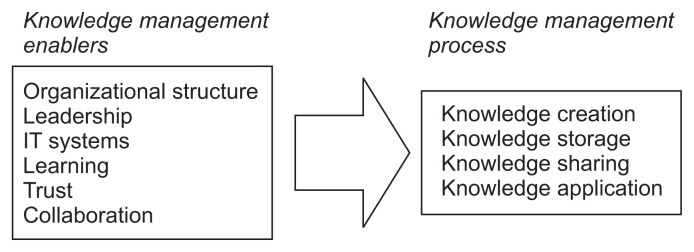
Table 1Background information of respondents
Table 2Results of factor analysis of constructs
Table 3Results of knowledge management (KM) research (multiple answers)
Table 4Results of the multiple regression analysis for the hospital A sample
| Hospital A sample | Knowledge creation beta | Knowledge storage beta | Knowledge sharing beta | Knowledge application beta |
|---|---|---|---|---|
| Organizational structure | 0.134 | 0.060 | −0.085 | 0.006 |
| Leadership | 0.023 | 0.161 | 0.143* | 0.121 |
| Information technology systems | 0.127 | 0.129 | 0.121 | 0.262*** |
| Learning | 0.052 | 0.047 | 0.127 | 0.047 |
| Truth | 0.175* | 0.061 | 0.193* | 0.055 |
| Collaboration | 0.050 | −0.041 | 0.065 | 0.002 |
| R2 | 0.181*** | 0.134*** | 0.286*** | 0.236*** |
Table 5Results of the multiple regression analysis for the hospital B sample
| Hospital B sample | Knowledge creation beta | Knowledge storage beta | Knowledge sharing beta | Knowledge application beta |
|---|---|---|---|---|
| Organizational structure | −0.124 | −0.035 | 0.065 | 0.155 |
| Leadership | 0.192* | 0.177* | 0.119 | 0.008 |
| Information technology systems | −0.077 | 0.276** | 0.004 | 0.019 |
| Learning | 0.082 | −0.142 | −0.032 | 0.017 |
| Truth | 0.020 | −0.172 | 0.058 | 0.053 |
| Collaboration | 0.267*** | 0.205* | 0.186* | 0.173* |
| R2 | 0.154*** | 0.110** | 0.101** | 0.098** |
Table 6Results of the multiple regression analysis for the hospital C sample
| Hospital C sample | Knowledge creation beta | Knowledge storage beta | Knowledge sharing beta | Knowledge application beta |
|---|---|---|---|---|
| Organizational structure | 0.008 | −0.029 | −0.017 | −0.108 |
| Leadership | 0.050 | 0.162 | 0.182* | 0.117 |
| Information technology systems | 0.164* | 0.051 | 0.026 | 0.194** |
| Learning | 0.023 | 0.124 | 0.126 | 0.113 |
| Truth | 0.099 | −0.067 | 0.072 | 0.088 |
| Collaboration | 0.137 | 0.136 | 0.195* | 0.150* |
| R2 | 0.210*** | 0.152*** | 0.262*** | 0.357*** |
Table 7Results of the multiple regression analysis for the hospital D sample
| Hospital D sample | Knowledge creation beta | Knowledge storage beta | Knowledge sharing beta | Knowledge application beta |
|---|---|---|---|---|
| Organizational structure | 0.021 | −0.040 | 0.008 | 0.011 |
| Leadership | 0.180* | 0.208** | 0.142* | 0.141* |
| Information technology systems | 0.173* | 0.232** | 0.151* | 0.245** |
| Learning | 0.023 | 0.025 | 0.081 | −0.037 |
| Truth | 0.069 | 0.201** | 0.285*** | 0.182** |
| Collaboration | 0.088 | −0.035 | 0.004 | 0.082 |
| R2 | 0.253*** | 0.303*** | 0.392*** | 0.318*** |
Figure & Data
References
Citations
Citations to this article as recorded by 
- Knowledge management effects and performance in health care: a systematic literature review
Ritva Kosklin, Johanna Lammintakanen, Tuula Kivinen
Knowledge Management Research & Practice.2023; 21(4): 738. CrossRef - Knowledge Sharing through Social Media Platforms in the Silicon Age
Muhammad Yaqub, Abdullah Alsabban
Sustainability.2023; 15(8): 6765. CrossRef - Success factors for evidence-based healthcare practice adoption
Lovemore Motsi, Bester Chimbo
SA Journal of Information Management.2023;[Epub] CrossRef - Leadership, healthcare and knowledge management
Guilherme Agnolin, Lúcia Worma, Édis Mafra Lapolli, Cristiano José Castro de Almeida Cunha
International Journal for Innovation Education and.2022; 10(10): 61. CrossRef - Alignment of knowledge management process with clinical process to support evidence based decision in healthcare improvements: The case of selected Ethiopian hospitals
Mniyichel Belay, Amare Desta, Steve Smithson, Million Meshesha
Knowledge and Process Management.2021; 28(1): 3. CrossRef - Knowledge management enablers affecting patient care: The perspective of registered nurses in South West Nigeria
Olateju J. Ajanaku, Stephen Mutula
SA Journal of Information Management.2021;[Epub] CrossRef - A gestão do conhecimento em contexto hospitalar: uma scoping review
Andreia Mesquita, Diana Santos, Vítor Raposo
Revista de Investigação & Inovação em Saúde.2021;[Epub] CrossRef - Structural Equation Modeling to Explore the Relationship Between Organizational Culture Dimensions and Implementation of Knowledge Management in Teaching Hospitals
Ahmad Rahbar, Amir Ashkan Nasiripour, Mahmood Mahmoodi-Majdabadi
Health Scope.2020;[Epub] CrossRef - Improvement of Innovation Ability of Hospital Managers and Construction of Competitive Strategy
Li Han, Jing Li, Wenfeng Chen
International Journal of Circuits, Systems and Sig.2020; 14: 751. CrossRef - Modeling the Pathways of Knowledge Management Towards Social and Economic Outcomes of Health Organizations
Ion Popa, Simona Ștefan
International Journal of Environmental Research an.2019; 16(7): 1114. CrossRef - Implementation of Knowledge Management in Chinese Hospitals
Qiao-yuan Yan, Fei Xiang, Xiao-xu Shi, Qin Zhu
Current Medical Science.2018; 38(2): 372. CrossRef
 PubReader
PubReader Cite
Cite
