
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 8(1); 2017 > Article
-
Original Article
Estimating Tuberculin Skin Test Reactions among Children and Teenagers Who Received the Bacillus Calmette-Guerin Vaccination at Birth: A Meta-analysis - Mohammad Sadegh Rezaia, Siavosh Abedib, Mahdi Afsharic, Mahmood Moosazadehd
-
Osong Public Health and Research Perspectives 2017;8(1):3-10.
DOI: https://doi.org/10.24171/j.phrp.2017.8.1.02
Published online: February 28, 2017
aInfectious Diseases Research Center with Focus on Nosocomial Infection, Mazandaran University of Medical Sciences, Sari, Iran
bDepartment of Internal Medicine, Mazandaran University of Medical Sciences, Sari, Iran
cDepartment of Community Medicine, Zabol University of Medical Sciences, Zabol, Iran
dHealth Science Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran
- Corresponding author: Mahmood Moosazadeh, E-mail: mmoosazadeh1351@gmail.com
Copyright © 2017 Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
-
Objectives
- Tuberculin skin reaction size is one indicator of bacillus Calmette-Guérin (BCG) vaccine efficacy and a way to diagnose latent infection. Several primary studies have examined this issue. Combining the results of these studies using a meta-analysis will provide reliable evidence regarding this indicator for policymakers. This study aimed to estimate the total frequency of different tuberculin skin test reactions among Iranian children and teenagers who received the BCG vaccination at birth.
-
Methods
- National and international databanks were searched using relevant keywords. After the search strategy was restricted and duplicates were excluded, the titles and abstracts of the remaining papers were screened. All included studies included healthy children who received the BCG vaccine without confirmed tuberculosis exposure. Heterogeneity of the results was assessed using the Cochrane test and I2 index showed the random effects model as the best model for estimating the pooled results.
-
Results
- We combined the results of 14 primary studies including purified protein derivative reaction test measures of 26,281 Iranian children. The frequencies (95% confidence intervals) of the reactions were 8.5% (6.2–10.8) for patients with a reaction size ≥ 10 mm, 29.9% (22.3–37.4) for a reaction size of 5–9 mm, and 60% (48.9–71.1) for a reaction size < 5 mm.
-
Conclusion
- Our study showed that large numbers of Iranian children and teens have no positive BCG vaccine reaction and a considerable number of children have been exposed to Mycobacterium tuberculosis.
- Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis (MBT) and rarely by Mycobacterium bovis that mainly involves the lungs. Although effective treatment regimens are being used widely, TB is one of the most important problems worldwide with an incidence of 12 million cases in 2011 [1–4]. The incidence of all TB cases and smear-positive cases in Iran during 2012 were reportedly 13.7 and 6.4 per 100,000 population, respectively [5,6].
- Children play a key role in the epidemiology and transmission of TB infection. They can become infected after exposure to smear-positive cases and develop active TB during their lives following any immune system impairment, malnutrition, stress, hormonal changes (especially in women), pregnancy, and elderly. Therefore, age group is of great importance in the TB control programs as a potential reservoir for MBT [7,8]. Bacillus Calmette-Guérin (BCG) vaccination is a simple method of providing a high degree of immune protection to those without a previous MBT infection. The BCG vaccine first used in 1928 should be prescribed in countries with high TB prevalence. This vaccine has been used in Iran since 1989 [1,9,10].
- The prophylactic effect of the BCG vaccine is under debate; however, since it prevents the disseminated and dangerous forms of TB disease and no other immune vaccines have been developed, the BCG vaccine is widely used worldwide [11]. In addition, although BCG is a safe vaccine, some adverse reactions such as cellulitis, abscess development at the injection site, regional lymphadenitis, and disseminated BCG infection have been reported [12].
- The tuberculin test, the most common method of BCG vaccination evaluation, is used as a diagnostic parameter for TB infection. The reports of average reaction sizes vary among countries. For example, the frequencies of a positive purified protein derivative (PPD) reaction in Ugandan adolescents, Indian children < 5 years of age, 11–18-year-old teenagers in South India, and Gambian school children were reportedly 16% [13], 20% [14], 12% [15], and 6.9% [16], respectively.
- Several primary studies have been performed in Iran to estimate the frequencies of positive PPD reactions among different age groups. Combining the various results of these studies using systematic review and meta-analytic methods [17–19] can provide more reliable evidence. Therefore, we aimed to estimate the pooled prevalence of positive PPD reactions in Iranian children and adolescents who received a BCG vaccination at birth.
INTRODUCTION
- 1. Search strategy
- All national (SID, Magiran, and Medlib) and international (PubMed, Google Scholar, Scopus, and Science Direct) databanks were electronically searched to identify relevant studies published between 1995 and January 31, 2016 using the following keywords and their Farsi equivalents: “prevalence,” “frequency,” “percent,” “latent tuberculosis infection,” “tuberculin skin test,” “TST,” “LTBI,” “LTI,” “purified protein derivative,” “PPD,” “tuberculin test,” “latent tuberculosis,” “cross-sectional study,” “descriptive study,” “longitudinal study,” “cohort study,” “Iran,” and “children.”
- Two researchers independently performed the search during February 2 to 18, 2016. They also investigated all references of the identified studies to increase the search sensitivity. Another researcher randomly evaluated the search results to identify any previously ignored study. To find unpublished materials, non-electronic evidence was also searched. Moreover, we interviewed relevant experts and research centers to identify any available grey literature.
- 2. Study selection
- Full texts or abstracts of all documents found during the primary search were obtained. Duplicate and irrelevant papers were excluded after investigation of the titles, abstracts, and full texts. We also investigated the results to identify and remove all duplicate studies.
- 3. Quality assessment
- All selected papers were quality assessed using a pre-designed checklist used in previous studies [20]. This checklist was designed based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist [21] and included 12 questions regarding different aspects of the methodology such as study type, sample size and sampling design, study population, data collection method and instruments, variable definition, statistical tests, study objectives, and illustration of the results based on the objectives. One score was assigned to each question and studies with at least eight scores [20] were entered into the final meta-analysis.
- 4. Data extraction
- Required data were extracted from the studies including title, first author name, study date and location, study type, sample size and sampling methods, average sample age and range, publication language, cut-off point of the PPD reaction size for latent TB infection, skin test measurement date, BCG vaccination status, exposure to active TB cases, study sample source (hospital or community), frequency of samples with different PPD reaction sizes (0–5, 6–9, or ≥ 10 mm). Extracted data were entered into an Excel spreadsheet (Microsoft, Redmond, WA, USA).
- 5. Inclusion criteria
- All Persian and English written papers with sufficient quality scores and reporting sample size and tuberculin skin test results among an Iranian population of patients < 18 years of age were included in the meta-analysis.
- 6. Exclusion criteria
- Studies did not report tuberculin skin test reactions, BCG vaccination status and sample size, those conducted among TB suspicious populations or TB-exposed populations and > 18-year-old populations, full text free abstracts presented in congresses, case reports, case control and experimental studies, and studies that did not obtain high enough quality scores were excluded from the meta-analysis.
- 7. Statistical analysis
- The data analyses were performed using Stata ver. 11 software (Stata Corporation, College Station, TX, USA). The standard error of the MBT infection prevalence was calculated using the binomial distribution formula. The Cochrane (Q) test and I2 index were used to determine the degree of heterogeneity among the results of the primary studies. Based on the heterogeneity indices, a random effects model was used to combine the point estimates. Factors that influenced the heterogeneity were investigated using meta-regression models. We also analyzed the results in the different subgroups such as publication date, study group, and publication language. Point prevalences of MBT infection were illustrated in a forest plot. In this graph, each box represents the weight of the study and the cross-lines indicate the 95% confidence intervals (CIs). Since this meta-analysis was used to estimate a single indicator, publication bias was not assessed.
MATERIALS AND METHODS
- The 9,643 studies initially identified were reduced to 463 after restriction of the search strategy. Moreover, 167 duplicates were removed. During the title/abstract review, 211 irrelevant studies were excluded. The full-text review revealed 71 irrelevant papers. One relevant study was identified during the backwards citation tracking process. Another paper did not achieve required quality score. Ultimately, 14 articles were identified as being eligible for the meta-analysis (Figure 1).
- The frequency of a positive PPD reaction was investigated among 26,281 Iranian children and adolescents. These studies were published from 1995 by Nilforooshan (17% prevalence of TB infection) to 2015 by Masomi Asl (3.8% prevalence of TB infection) and Raffiee (14.1% prevalence of TB infection) (Table 1). Healthy vaccinated children unexposed to active TB cases were recruited in all studies. Tuberculin test results were measured 48–72 hours after injection. All studies used five units of tuberculin (0.1 mL forearm intradermal injection).
- Minimum and maximum positive reactions (> 10 mm) in the primary studies varied from zero in the study by Sakha in 2008 among children aged 84–96 months to 26.3% in the study by Zehni in 2001 among children aged 132–168 months (Table 1).
- As illustrated in Figure 2, based on the random effects model, the prevalence of a positive reaction (> 10 mm) among Iranian children and adolescents was estimated to be 8.5% (95% CI, 6.2–10.8; I2, 98.4%; Q, 822.20; p < 0.001).
- Due to the considerable heterogeneity among the results of the primary studies, meta-regression model investigation of the “year of publication” variable showed a significant influence on heterogeneity (β = −0.8, p = 0.009) (Figure 3).
- The prevalence of positive reactions in the six studies conducted before 2008 was estimated to be 12.5% (95% CI, 5.6–19.5), while the prevalence in the eight studies performed after 2008 was estimated to be 5.8% (95% CI, 4.1–7.5). In addition, the frequency of positive reactions (≥ 10 mm) among children < 6 years of age was 10.7% (95% CI, 4.4–17), among children aged 6–16 years of age was 8.89% (95% CI, 5.3–12.7), and among those aged 3 months to 16 years was 5.5% (95% CI, 3.4–7.6). The observed overlaps between the confidence intervals for the different age groups indicated that these differences were not statistically significant (Figure 4).
- The prevalence of 5–9-mm skin reaction sizes among Iranian children was estimated to be 29.9% (95% CI, 22.3–37.4), while that for reactions sizes < 5 mm was 59.99% (95% CI, 48.9–71.1) (Figures 5 and 6).
RESULTS
- Our meta-analysis showed that 8.5% of Iranian children and teenagers with a history of BCG vaccination during the first 3 months of life had PPD skin reaction sizes ≥ 10 mm. Moreover, we found that about 60% of them showed no test reaction. Reaction sizes > 10 mm were more common in the recent than older studies.
- During a meta-analysis conducted in 2002 [22], the prevalence of a PPD reaction size > 10 mm was estimated to be 22.8% when combining the tuberculin skin test results in the USA, Canada, Queensland, and Spain. The corresponding rate for the survey results in the Philippines, Saudi Arabia, Solomon Island, South America, Turkey, and United Arab Emirates was 28.8%. These results are considerably higher than those estimated in the current study. One explanation for such variations is differences in the study samples. In these meta-analyses, the time gap between BCG vaccination and tuberculin testing was at least 5 years, while our study samples received the BCG vaccine at least 3 months prior to PPD testing. It seems that the greater the time interval between immunization and PPD testing, the greater the PPD reaction sizes would be observed. Wang et al [22] combined the results of different studies by time interval and estimated the prevalence of positive PPD skin test results for populations whose time gaps were < 15 years as of 12.6%, while the corresponding prevalence for those with a time gap > 15 years was estimated to be 47.2%. Age differences among populations can be another reason for such variations. The mean age in the Wang et al’s study populations was more than that in the current meta-analysis. In addition, the dates of tuberculin surveys are different in our study (1995–2015) from those in the study performed by Wang et al (1996–1999). Moreover, the prevalences of TB, malnutrition, HIV/AIDS, and other immunocompromised disorders differed among studies.
- The prevalence of positive tuberculin skin test reactions has been reported in many studies in different parts of the world, such as 16.1% in Ugandan adolescents [15], 20% in Indian children < 5 years of age [14], 12% among 11–18-year-old teenagers in southern India [14], and 6.9% in Gambian school children [16]. The reported prevalences in three studies [13–15] were higher than those of the current Iranian meta-analysis. Only the Gambian survey [16] showed lower estimates than Iran. Another survey of Chinese children > 5 years of age [23] reported an age-sex standardized prevalence of positive PPD tests of 15% to 42%, which was higher than our estimates.
- Marquez et al [24] reported a 24% prevalence of positive PPD tests among Ugandan children < 5 years of age. It was at most 36% among children in the first year of life and at least 19% in children aged 36–60 months. Both estimates are higher than ours. The higher prevalence of HIV/AIDS might explain such differences. Another study performed in southeast Iran showed significant differences in reaction sizes between the sexes but no difference among age groups [25].
- Many factors influence the tuberculin skin test reaction sizes including vaccine type and dose, vaccination age and time, history of MBT exposure, history of active TB exposure, time interval between BCG vaccination and PPD testing, children’s nutritional status, and PPD booster effect [26–28]. All of these factors can be reasons for the observed heterogeneity among the results of different tuberculin skin test surveys.
- Some of our TB-infected study samples might be due to exposure to untreated TB. Most of the samples showed no PPD reaction. Because of remarkable delays in TB diagnosis in Iran, these non-response groups are susceptible to developing TB. According to several studies conducted in Iran, there are notable delays in both diagnosis and treatment of TB patients. Alavi et al [29] showed that 65.5% of smear-positive TB cases in Khuzestan province started TB treatment after an average delay of 73 days. Another cross-sectional study in Iran reported a 59-day delay [30]. Since the low efficacy of BCG vaccination in TB prevention, such a delay can be an important potential source of new infections among children. Another study performed in Russia reported an increasing trend for TB infection from 0.2% in 1991 to 1.6% in 2000 [31].
- One of the limitations of the current study was its wide age range among the study populations, which could be a probable factor for unreliable results. In four studies, the sample age was 3–16 months made it difficult to analyze the results according to < 6-year-old and > 6-year-old age groups. The significant heterogeneity between the results of primary studies was another limitation of our meta-analysis. Therefore, we applied the random effects model to combine the results. We also did not report the pooled results based on sex because such sub-analyses had not been reported in the primary studies. However, using the cut-off point method as an indicator of TB infection prevalence is prone to challenges, and more reliable methods for interpreting PPD skin reactions were applied in some of the primary studies that reported different results [32].
- Our study revealed that a major proportion of Iranian children and adolescents had no positive reaction after BCG vaccination, whereas some had latent TB infection. Results of this study showed an acceptable view of BCG efficacy and latent TB infection among these age groups. Note that early case detection and treatment is the most effective strategy for controlling TB infection and disease and that reinforcement of case finding and control programs can help achieving these strategies. Future similar studies among limited age ranges of populations are needed to confirm our results.
DISCUSSION
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
Article information
- 1. Sayyahfar S, Karimi A, Fahimzad A, et al. Comparison of Tuberculin Skin Test result and interferon gamma response to human PPD in BCG scar positive and negative children. J Epidemiol Glob Health 2014;4:45−50. https://doi.org/10.1016/j.jegh.2013.09.002. PMID: 10.1016/j.jegh.2013.09.002. PMID: 24534335.ArticlePubMed
- 2. Moosazadeh M, Khanjani N, Nasehi M, et al. Predicting the incidence of smear positive tuberculosis cases in Iran using time series analysis. Iran J Public Health 2015;44:1526−34. PMID: 26744711.PubMedPMC
- 3. Moosazadeh M, Bahrampour A, Nasehi M, et al. The incidence of recurrence of tuberculosis and its related factors in smear-positive pulmonary tuberculosis patients in Iran: a retrospective cohort study. Lung India 2015;32:557−60. https://doi.org/10.4103/0970-2113.168113. PMID: 10.4103/0970-2113.168113. PMID: 26664159.ArticlePubMedPMC
- 4. Moosazadeh M, Nezammahalleh A, Movahednia M, et al. Predictive factors of death in patients with tuberculosis: a nested case-control study. East Mediterr Health J 2015;21:287−92. PMID: 26077524.ArticlePubMed
- 5. Nasehi MM, Moosazadeh M, Amiresmaeili MR, et al. The epidemiology of factors associated with screening and treatment outcomes of patients with smear positive pulmonary tuberculosis: a population-based study. J Mazand Univ Med Sci 2012;21:9−18.
- 6. Moosazadeh M, Nasehi M, Bahrampour A, et al. Forecasting tuberculosis incidence in iran using box-jenkins models. Iran Red Crescent Med J 2014;16:e11779https://doi.org/10.5812/ircmj.11779. PMID: 10.5812/ircmj.11779. PMID: 25031852.ArticlePubMedPMC
- 7. Reed C, von Reyn CF, Chamblee S, et al. Environmental risk factors for infection with Mycobacterium avium complex. Am J Epidemiol 2006;164:32−40. https://doi.org/10.1093/aje/kwj159. PMID: 10.1093/aje/kwj159. PMID: 16675537.ArticlePubMed
- 8. Getahun H, Matteelli A, Abubakar I, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J 2015;46:1563−76. https://doi.org/10.1183/13993003.01245-2015. PMID: 10.1183/13993003.01245-2015. PMID: 26405286.ArticlePubMedPMC
- 9. Jason J, Archibald LK, Nwanyanwu OC, et al. Clinical and immune impact of Mycobacterium bovis BCG vaccination scarring. Infect Immun 2002;70:6188−95. https://doi.org/10.1128/IAI.70.11.6188-6195.2002. PMID: 10.1128/IAI.70.11.6188-6195.2002. PMID: 12379697.ArticlePubMedPMC
- 10. Rezai MS, Khotaei G, Mamishi S, et al. Disseminated Bacillus Calmette-Guerin infection after BCG vaccination. J Trop Pediatr 2008;54:413−6. https://doi.org/10.1093/tropej/fmn053. PMID: 10.1093/tropej/fmn053. PMID: 18593737.ArticlePubMed
- 11. Colditz GA, Berkey CS, Mosteller F, et al. The efficacy of bacillus Calmette-Guérin vaccination of newborns and infants in the prevention of tuberculosis: meta-analyses of the published literature. Pediatrics 1995;96:29−35. PMID: 7596718.PubMed
- 12. Shahmohammadi S, Saffar MJ, Rezai MS. BCG-osis after BCG vaccination in immunocompromised children: case series and review. J Pediatr Rew 2014;2:47−54. https://doi.org/10.7508/JPR-V2-N1-62-74.Article
- 13. Mumpe-Mwanja D, Verver S, Yeka A, et al. Prevalence and risk factors of latent Tuberculosis among adolescents in rural Eastern Uganda. Afr Health Sci 2015;15:851−60. https://doi.org/10.4314/ahs.v15i3.20. PMID: 10.4314/ahs.v15i3.20. PMID: 26957974.ArticlePubMedPMC
- 14. Jain SK, Ordonez A, Kinikar A, et al. Pediatric tuberculosis in young children in India: a prospective study. Biomed Res Int 2013;2013:783698https://doi.org/10.1155/2013/783698. PMID: 10.1155/2013/783698. PMID: 24386640.ArticlePubMedPMC
- 15. Uppada DR, Selvam S, Jesuraj N, et al. The tuberculin skin test in school going adolescents in South India: associations of socio-demographic and clinical characteristics with TST positivity and non-response. BMC Infect Dis 2014;14:571https://doi.org/10.1186/s12879-014-0571-7. PMID: 10.1186/s12879-014-0571-7. PMID: 25927335.ArticlePubMedPMC
- 16. Adetifa IM, Muhammad AK, Jeffries D, et al. A Tuberculin skin test survey and the annual risk of mycobacterium tuberculosis infection in gambian school children. PLoS One 2015;10:e0139354https://doi.org/10.1371/journal.pone.0139354. PMID: 10.1371/journal.pone.0139354. PMID: 26465745.ArticlePubMedPMC
- 17. Moosazadeh M. Meta-analysis of prevalence of smoking in 15–64-year-old population of west of Iran. Int J Prev Med 2013;4:1108−14. PMID: 24319549.PubMedPMC
- 18. Amiresmaili M, Moosazadeh M. Determining job satisfaction of nurses working in hospitals of Iran: a systematic review and meta-analysis. Iran J Nurs Midwifery Res 2013;18:343−8. PMID: 24403934.PubMedPMC
- 19. Moosazadeh M, Amiresmaili M, Aliramezany M. Prevalence of G6PD deficiency in Iran, a mata-analysis. Acta Med Iran 2014;52:256−64. PMID: 24901854.PubMed
- 20. Moosazadeh M, Nekoei-Moghadam M, Emrani Z, et al. Prevalence of unwanted pregnancy in Iran: a systematic review and meta-analysis. Int J Health Plann Manage 2014;29:e277−90. https://doi.org/10.1002/hpm.2184. PMID: 10.1002/hpm.2184. PMID: 23630092.ArticlePubMed
- 21. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg 2014;12:1500−24. https://doi.org/10.1016/j.ijsu.2014.07.014. PMID: 10.1016/j.ijsu.2014.07.014. PMID: 25046751.ArticlePubMed
- 22. Wang L, Turner MO, Elwood RK, et al. A meta-analysis of the effect of Bacille Calmette Guérin vaccination on tuberculin skin test measurements. Thorax 2002;57:804−9. PMID: 10.1136/thorax.57.9.804. PMID: 12200526.ArticlePubMedPMC
- 23. Gao L, Lu W, Bai L, et al. Latent tuberculosis infection in rural China: baseline results of a population-based, multicentre, prospective cohort study. Lancet Infect Dis 2015;15:310−9. https://doi.org/10.1016/S1473-3099(14)71085-0. PMID: 10.1016/S1473-3099(14)71085-0. PMID: 25681063.ArticlePubMed
- 24. Marquez C, Chamie G, Achan J, et al. Tuberculosis infection in early childhood and the association with HIV-exposure in HIV-uninfected children in rural uganda. Pediatr Infect Dis J 2016;35:524−9. https://doi.org/10.1097/INF.0000000000001062. PMID: 10.1097/INF.0000000000001062. PMID: 26771662.ArticlePubMedPMC
- 25. Afshari M, Baneshi MR, Haghdoost AA. Comparing the results of cut-off method, anti-mode method and mirror image method in estimating the prevalence of tuberculosis infection. Health Med J 2013;7:3103−10.
- 26. Uyan AP, Baskin E, Büyükbese E, et al. Evaluating Bacillus-Calmette-Guerin vaccination by tuberculin skin test response. Indian Pediatr 2000;37:1106−10. PMID: 11042711.PubMed
- 27. Camlar SA, Makay B, Appak O, et al. Performance of tuberculin skin test and interferon gamma assay for the diagnosis of latent tuberculosis infection in juvenile idiopathic arthritis. Clin Rheumatol 2011;30:1189−93. https://doi.org/10.1007/s10067-011-1724-3. PMID: 10.1007/s10067-011-1724-3. PMID: 21403997.ArticlePubMed
- 28. Moosazadeh M, Khanjani N, Parsaee M. The prevalence of latent tuberculosis infection and smear positive pulmonary tuberculosis in people with household close contact with tuberculosis in north of iran. Iran J Med Sci 2015;40:161−5. PMID: 25821296.PubMedPMC
- 29. Alavi SM, Bakhtiyariniya P, Albagi A. Factors associated with delay in diagnosis and treatment of pulmonary tuberculosis. Jundishapur J Microbiol 2015;8:e19238https://doi.org/10.5812/jjm.19238. PMID: 10.5812/jjm.19238. PMID: 25861434.ArticlePubMedPMC
- 30. Nasehi M, Hassanzadeh J, Rezaianzadeh A, et al. Diagnosis delay in smear positive tuberculosis patients. J Res Med Sci 2012;17:1001−4. PMID: 23833571.PubMedPMC
- 31. Yuen CM, Krapivina TM, Kazennyy BY, et al. Annual risk of tuberculous infection measured using serial skin testing, Orel Oblast, Russia, 1991–2005. Int J Tuberc Lung Dis 2015;19:39−43. https://doi.org/10.5588/ijtld.14.0445. PMID: 10.5588/ijtld.14.0445.Article
- 32. Haghdoost AA, Afshari M, Baneshi MR, et al. Estimating the annual risk of tuberculosis infection and disease in southeast of Iran using the bayesian mixture method. Iran Red Crescent Med J 2014;16:e15308https://doi.org/10.5812/ircmj.15308. PMID: 10.5812/ircmj.15308. PMID: 25593722.ArticlePubMedPMC
REFERENCES
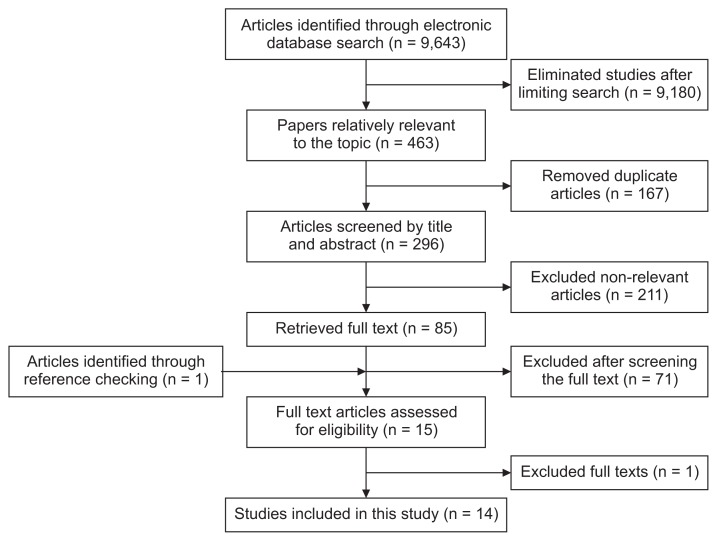
Figure 2
Point and pooled prevalences of the tuberculin skin test reaction (≥ 10 mm) among Iranian children and adolescents according to the results of primary studies before and after 2008.
ES, effect size; CI, confidence interval.
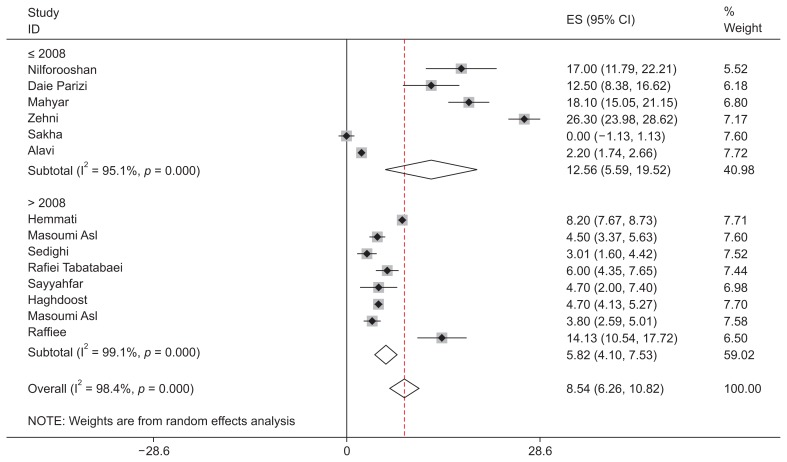
Figure 3
Investigating “publication year” as a heterogeneity factor on meta-regression analysis.
PPD, purified protein derivative.
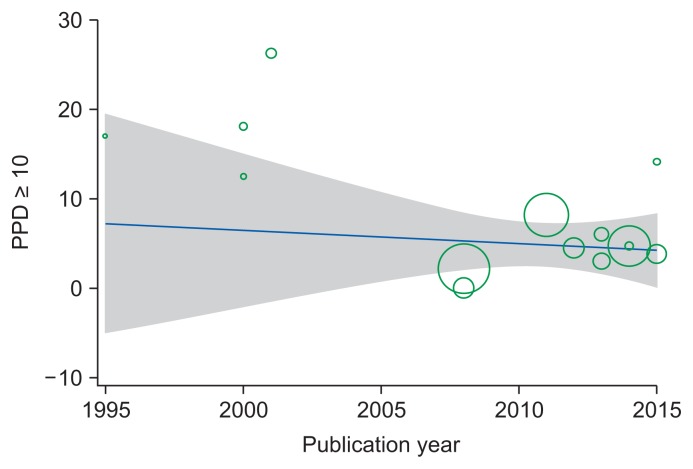
Figure 4
Point and pooled prevalences of the tuberculin skin test reaction (≥ 10 mm) among Iranian children and adolescents by different age groups.
ES, effect size; CI, confidence interval.

Figure 5
Point and pooled prevalences of 5–9-mm tuberculin skin reaction size among Iranian children and adolescents.
ES, effect size; CI, confidence interval.
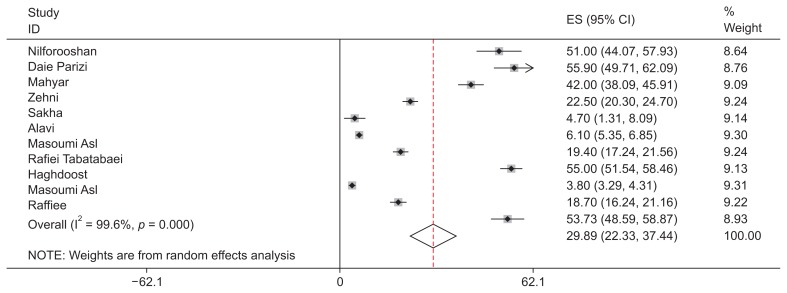
Figure 6
Point and pooled prevalences of <5 mm tuberculin skin reaction sizes among Iranian children and adolescents.
ES, effect size; CI, confidence interval.
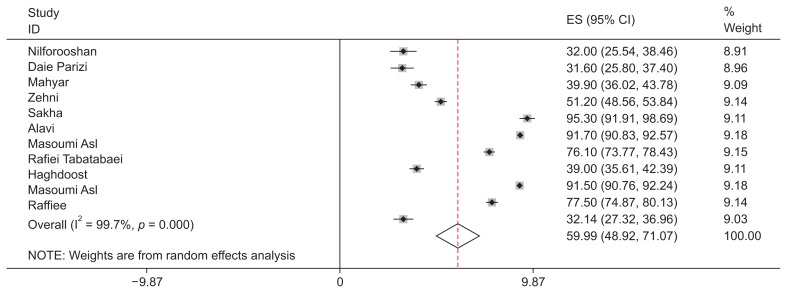
Table 1Characteristics of primary studies included in the meta-analysis
Figure & Data
References
Citations
Citations to this article as recorded by 
- Comparison of Serum Immunoglobulin Levels and Lymphocyte Counts in Children with Lymphadenitis Following BCG Vaccination
Leila Barati, Arash Kalantari, Jalaladdin Sheikh, Fateme-Sadat Tabatabaee, Farshid Kompani, Maryam Najafinejad, Ahmad Sohrabi, Fatemeh Cheraghali
Iranian Journal of Pediatrics.2022;[Epub] CrossRef - Is latent tuberculosis infection challenging in Iranian health care workers? A systematic review and meta-analysis
Mohammad Hossein YektaKooshali, Farahnaz Movahedzadeh, Ali Alavi Foumani, Hoda Sabati, Alireza Jafari, HASNAIN SEYED EHTESHAM
PLOS ONE.2019; 14(10): e0223335. CrossRef
 PubReader
PubReader Cite
Cite





