Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 11(5); 2020 > Article
-
Brief Report
Air Evacuation of Passengers with Potential SARS-CoV-2 Infection Under the Guidelines for Appropriate Infection Control and Prevention - Jeong-Gil Kima, Seung Hak Leeb, Hansuk Kimc, Hong Sang Ohd, Jacob Leee
-
Osong Public Health and Research Perspectives 2020;11(5):334-338.
DOI: https://doi.org/10.24171/j.phrp.2020.11.5.10
Published online: October 22, 2020
aMedical Department, Armed Forces Yangju Hospital, Yangju, Korea
bDepartment of Rehabilitation Medicine, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, Korea
cIncheon Airport National Quarantine Station, Incheon, Korea
dDivision of Infectious Disease, Department of Internal Medicine, Armed Forces Capital Hospital, Seongnam, Korea
eDivision of Infectious Diseases, Department of Internal Medicine, College of Medicine, Hallym University, Chuncheon, Korea
- *Corresponding author: Jacob Lee, Division of Infectious Diseases, Department of Internal Medicine, College of Medicine, Hallym University, Chuncheon, Korea, E-mail: litjacob@gmail.com
• Received: September 1, 2020 • Revised: September 23, 2020 • Accepted: September 24, 2020
Copyright ©2020, Korea Centers for Disease Control and Prevention
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
- This report describes the air evacuation of 80 Koreans from Iran to Korea on March 19th, 2020, with a direct transfer of passengers between airplanes in Dubai. The passengers were potentially infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) so, strict precautions were taken for the duration of the flight, and the passengers were screened before embarking from Dubai and disembarking at Incheon International Airport in Korea. Passengers with fever or symptoms of SARS-CoV-2 were assessed by a quarantine doctor, and if they were suspected of being infected with SARS-CoV-2, they were categorized as a “patient under investigation (PUI)”. There was 1 passenger designated as a PUI before the departure from Dubai and another designated as a PUI upon arrival into Korea. The first PUI tested negative, but the second PUI tested positive for SARS-CoV-2. All those aboard the flight (passengers, aircrew, and medical staff) were screened for SARS-CoV-2 upon arrival into Korea and completed a mandatory 14-day medical quarantine. There were no additional cases of infection.
- On March 11th, 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) a pandemic [1]. Following this announcement, countries around the world started to evacuate their residents overseas. Koreans were successfully repatriated from several foreign countries where there was a COVID-19 epidemic [2,3]. Unlike the previous Chinese and Japanese evacuations, which were short-haul flights, the evacuation of 80 Koreans from Iran was more challenging [4] because of additional safety precautions (e.g., separating seats, dividing zones, and managing the use of toilets on board the aircraft). The evacuees were moved from Tehran in Iran to Al Maktoum International Airport in Dubai via an Iranian aircraft on March 19th, 2020. A doctor was dispatched to be in charge of transport quarantine for flights from Tehran to Incheon. To our knowledge, there are no published reports on air transport according to the World Health Organization air transport guidelines, of a large group of potentially infectious individuals [5].
- 1. Zoning
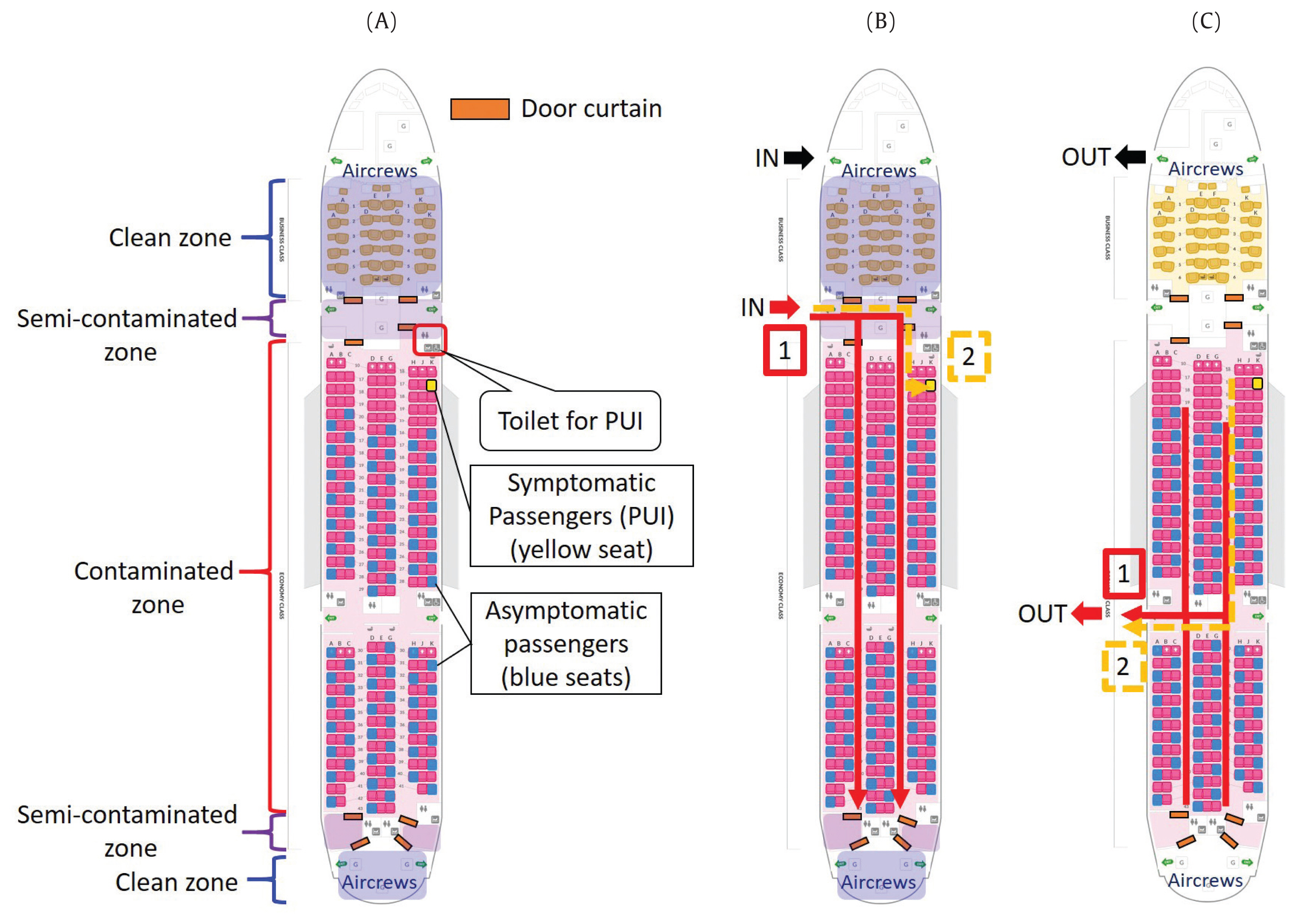
- The Korean government selected the Boeing 777-200 aircraft as a charter plane to accommodate the number of residents required to be repatriated to Korea. The first-class seats in the front were designated as a clean zone, and the economy seats in the middle and rear were designated as a contaminated zone (Figure 1A).
- There were 8 sets of transparent vinyl curtains with inside magnets installed in the aircraft to separate the clean and contaminated zones, with a semi-contaminated zone in the middle (Figure 2). The medical staff and the flight crew took off their personal protective equipment (PPE) in the semi-contaminated zone and moved into the clean zone. The vinyl curtains were attached with double-sided adhesive tape, which created an air seal.
- In the Boeing 777-200, there are 3 seats per row, and 2 seats in the back row (Figure 1A). The asymptomatic passengers were seated in a zigzag formation to minimize the risk of droplet propagation through the air, from the patient sat behind. Symptomatic passengers were seated in the front of the aircraft, maintaining sufficient distance from the asymptomatic passengers, and enabling medical staff to access symptomatic passengers without passing asymptomatic passengers.
- 2. Pre-transfer quarantine
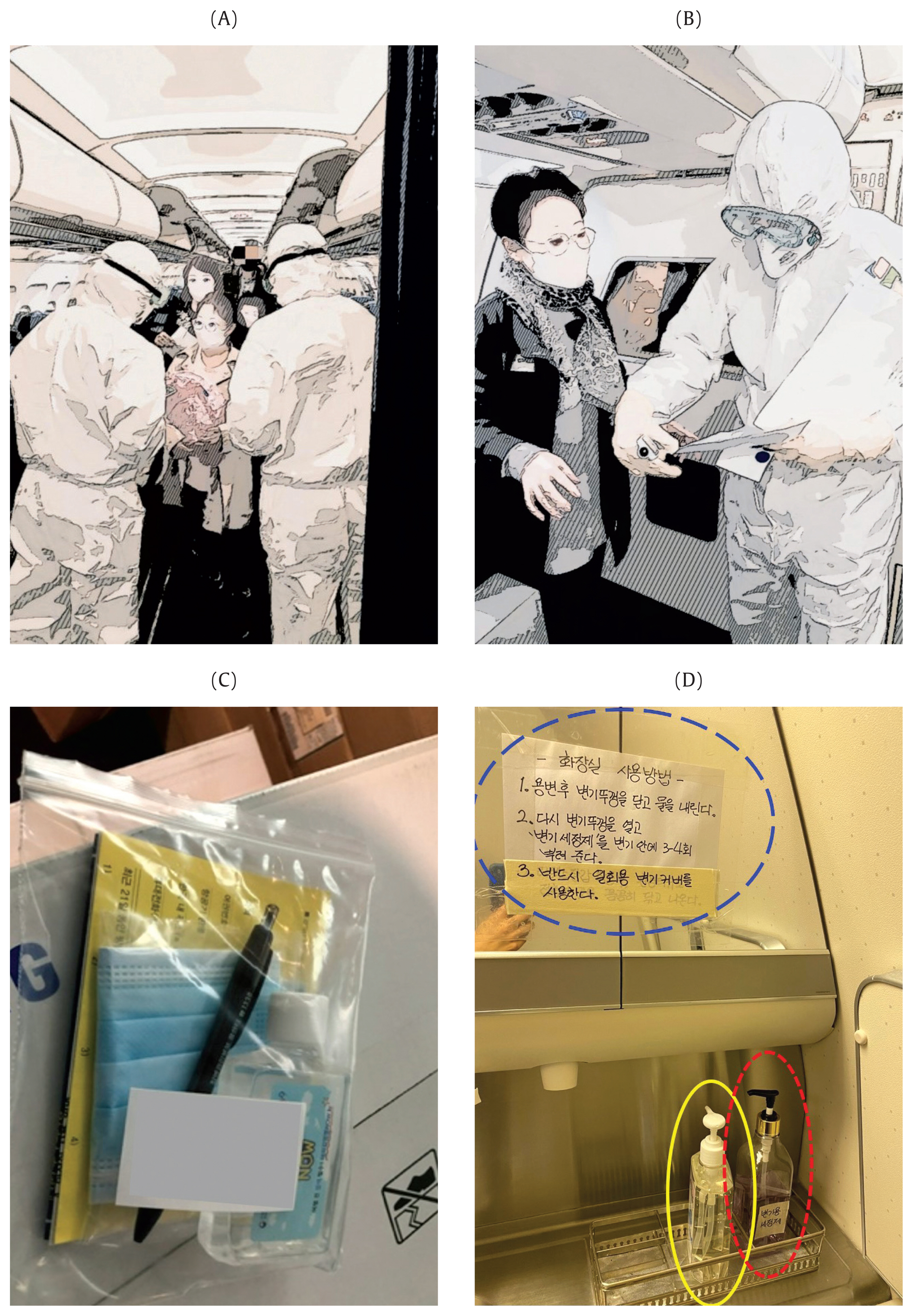
- When the Iranian aircraft had parked alongside the Korean aircraft, 2 quarantine officers and a quarantine doctor wearing PPE entered the Iranian aircraft via a vehicle mounted scissor lift platform. The quarantine process was explained via the intercom on the aircraft, and the pre-filled Health Status Questionnaires (HSQs) and passengers’ body temperature were taken (Figure 3A). Passengers who reported respiratory symptoms in the previous 14 days on the HSQ or who had a temperature of ≥ 37.5°C were immediately assessed for COVID-19 by the quarantine doctor (Figure 3B). Passengers had a blue or a red sticker placed on their chest, depending on whether they were asymptomatic or under investigation, respectively, so that their COVID-19 status could be easily identified. One passenger with a mild sore throat and myalgia 2 weeks previously, who had a temperature of 37.9°C was categorized as a patient under investigation (PUI) by the quarantine doctor.
- 3. Passenger transfer, movement control, and education
- Asymptomatic passengers disembarked from the Iranian aircraft first and moved to the Korean aircraft staying at least 2 meters apart from each other. A nurse stationed at the entry to the vehicle mounted scissor lift platform disinfected passengers’ hands, replaced their facemasks, and gave each passenger a package containing a hand sanitizer, an inflight behavior guide, a new HSQ, a pen, and an extra face mask (Figure 3C). The crew assigned passengers’ seats prior to the passengers entering the aircraft to ensure optimal separation as passengers entered the front of the aircraft. The PUI boarded last and was assigned a prepared seat close to the entrance to the aircraft (Figure 1B).
- The quarantine doctor provided instructions on in-flight infection control practices before take-off. These included remaining seated (except when using the toilet), wearing a facemask (except during mealtimes), and frequently using the hand sanitizer provided. Passengers were instructed on how to use the toilet, using a disposable seat cover, closing the toilet to flush, reopening it, and pumping 3–4 squirts of dilute sodium hypochlorite into the toilet bowl (Figure 3D). Passengers were instructed to wipe all the places that they touched with dilute sodium hypochlorite (dispensed onto a tissue). The PUI was given acetaminophen (paracetamol) 650 mg (× 4) to use if symptoms became severe.
- 4. Air-conditioning, designated toilets for symptomatic passengers, and in-flight services
- Air flow into the engine is sterilized through the engine compressor, cooled, and flows into the cabin from above through a high-efficiency particulate air filter, so the air entering the cabin is relatively safe [6]. A toilet located nearby the designated symptomatic passenger seats, was assigned to the PUI (Figure 1A). For infection control, a meal, a snack, and sufficient water were provided in advance individually wrapped in a plastic bag to minimize the need for inflight service. The crew members who attended to the asymptomatic passengers wore N95 masks, gloves, and plastic vinyl aprons, and the crew members and medical staff who attended to the PUI wore Level D PPE. To ensure a safe long distance flight, the quarantine doctor taught the aircrew how to put-on and take-off the PPE, how to clean the cabin, and how to maintain personal hygiene before departing from Korea and Dubai.
- 5. Disembarking, airport quarantine, and medical waste disposal and cleaning
- To exit the plane passengers left from back of the aircraft (Figure 1C). The asymptomatic passengers exited first, and received a pre-quarantine screening at the arrival gate. The waiting quarantine officers checked the pre-filled HSQs, measured passengers’ body temperatures, and asked them about symptoms they experienced during the flight. Based on this screening, 1 additional passenger was categorized as a PUI on arrival.
- The 2 PUIs were transported (using a prepared ambulance) to a negative-pressure isolation facility at Incheon International Airport Quarantine Station. The asymptomatic passengers had a respiratory swab collected for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing performed in a mobile laboratory outside the airport, and were transported individually to separate isolation quarters. The 2 PUIs had diagnostic samples collected in their isolated rooms at the quarantine facility. After all the passengers had disembarked from the aircraft, the quarantine doctor and a nurse wearing PPE, collected all the garbage left by the passengers, removed the vinyl curtains, and disposed them in a medical waste container. They also collected the medical waste including the protective clothing, gloves, and masks used in the semi-contaminated zone, and an infectious disease cleaning company was commissioned to disinfect the cabin.
Introduction
- The passenger identified as a PUI on the flight from Iran tested negative for SARS-CoV-2, but the passenger who developed a fever during flight from Dubai to Korea was confirmed as positive for SARS-CoV-2. No additional passengers, aircrew, medical staff, or others involved in the evacuation, developed signs of infection during the 14-day observation period.
Results
- Several studies related to inflight infections have been published [6–8]. Most studies have dealt with the inflight mechanism of transmission, the effect of air conditioning on infectivity, and the effectiveness of wearing facemasks during a flight. This is the first practical account of prevention of infectious disease transmission in a high-risk group, during air evacuation, using full infection control and prevention measures.
- The first PUI was determined not to be infected with SARS-CoV-2, but the second PUI tested positive for SARS-CoV-2. All those aboard the flight (passengers, aircrew, and medical staff) were screened for SARS-CoV-2 upon arrival in Korea and completed a mandatory 14-day medical quarantine. This account illustrates that transmission of infection can be controlled in long-distance flights if the aircraft cabin is thoroughly prepared in hospital infection control and prevention standards.
- We hope that this account will serve as a guideline for infection control and prevention during future air evacuations during international infectious disease epidemics.
Discussion
-
Acknowledgements
- I wish to express my deepest gratitude to nurse Hyomin Lee, and quarantine officers Bomi Kim and Ji Eon Kim for carrying out this air evacuation.
Acknowledgments
- 1. World Health Organization [Internet]. WHO announces COVID-19 outbreak a pandemic [cited 2020 Mar 12]. Available from: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
- 2. Yonhap News [Internet]. South Korea to send third flight to Wuhan to bring home Korean nationals, families [cited 2020 Feb 9]. Available from: https://en.yna.co.kr/view/AEN20200209003552325.
- 3. The Japan Times [Internet]. South Korea to send plane to evacuate citizens from quarantined Diamond Princess cruise ship [cited 2020 Feb 18]. Available from: https://www.japantimes.co.jp/news/2020/02/18/national/science-health/south-korea-evacuate-diamond-princess/#.XpPCY1MzY1I.
- 4. Yonhap News [Internet]. S. Korean chartered flight heads home carrying 80 people evacuated from coronavirus-hit Iran [cited 2020 Mar 19]. Available from: https://en.yna.co.kr/view/AEN20200318006452325.
- 5. Handbook for the Management of Public Health Events in Air Transport. Geneva (Switzerland): World Health Organization; 2015. p 98.
- 6. Gupta JK. Respiratory exhalation/inhalation models and prediction of airborne infection risk in an aircraft cabin. West Lafayette (IL): Purdue University; 2010.
- 7. Withers MR, Christopher GW, Hatfill SJ, et al. Aeromedical evacuation of patients with contagious infections. Aeromedical Evacuation. New York (NY): Springer; 2003. pp 147−59. PMID: 10.1007/0-387-22699-0_11.Article
- 8. Wan MP, Sze To GN, Chao CYH, et al. Modeling the Fate of Expiratory Aerosols and the Associated Infection Risk in an Aircraft Cabin Environment. Aerosol Sci Technol 2009;43(4). 322−43. PMID: 10.1080/02786820802641461.Article
References
Figure 1
(A) The seat map for the Boeing 777-200 aircraft. The first-class seats in the front of aircraft had to be designated as a clean zone and the economy seats in the middle and rear were set as a contaminated zone to control infection on board. In addition, a clean zone and a contaminated zone were divided by using 2 curtain-type transparent vinyl doors, and a semi-contaminated zone was established between them. Asymptomatic passengers were seated in a zigzag form in 1 row to minimize the risk of droplet propagation from the rear seat, and symptomatic passengers were seated in front contaminated zone with sufficient space. The toilet for the patient under investigation (PUI) was set close to them.
(B) The route for passengers to board the aircraft. The solid red arrow and the yellow dotted arrow indicates the boarding route of asymptomatic and symptomatic passenger, respectively. Asymptomatic passengers boarded first, and then symptomatic passengers boarded.
(C) The route for passengers to disembark the aircraft. A different entrance was used when boarding. The solid red arrow and the yellow dotted arrow indicates the route for disembarking asymptomatic and symptomatic passenger, respectively. Asymptomatic passengers disembarked first, followed by symptomatic passengers.
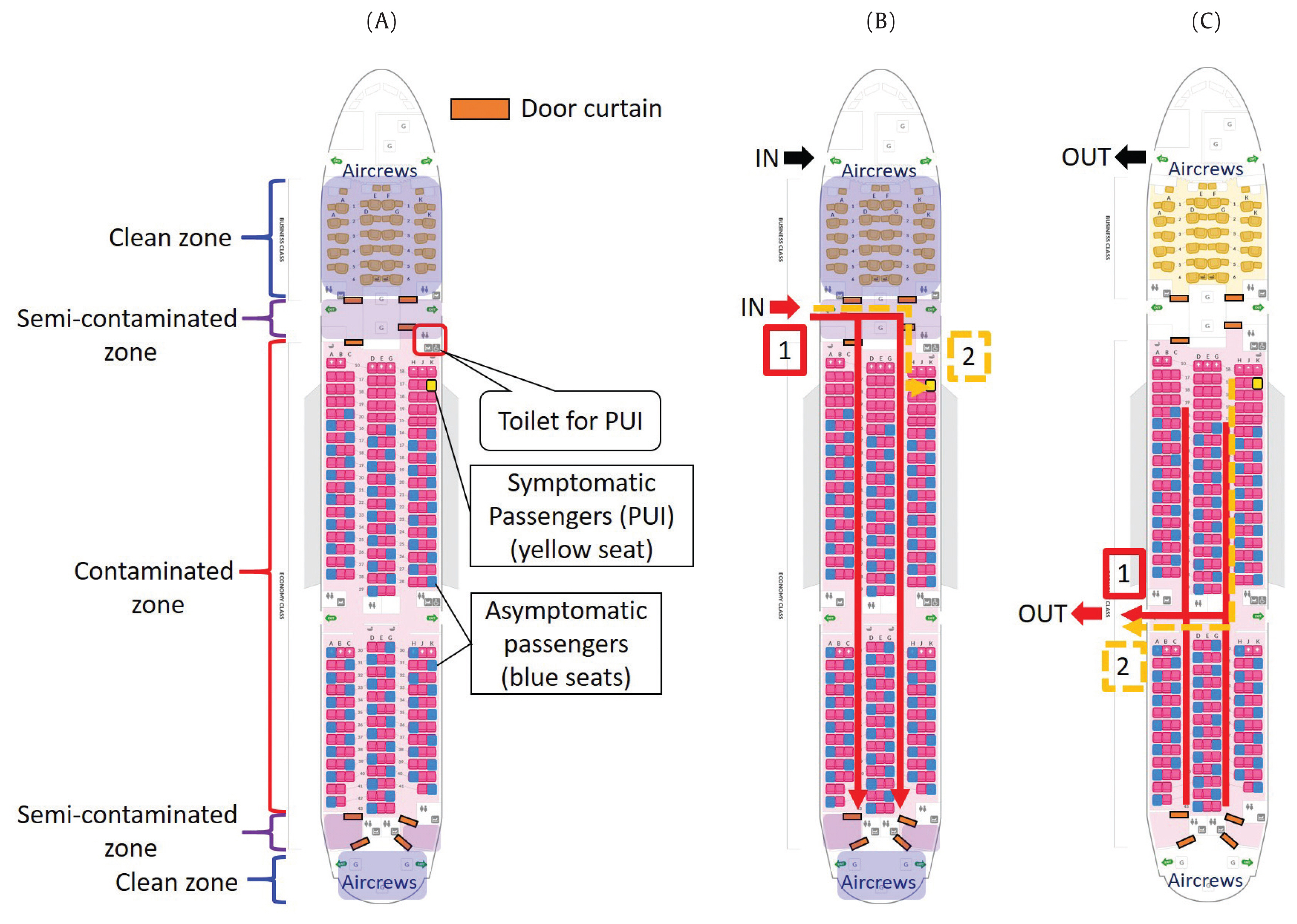
Figure 2Vinyl curtain doors. The doors were attached with a double-sided adhesive tape. The center contains a magnet, so when people push, the magnetic door opens, and closes automatically.

Figure 3
(A) Pre-transfer quarantine. Two quarantine officers collected pre-filled Health Status Questionnaires (HSQ) from the central aisle while simultaneously measuring body temperature.
(B) The passenger who had respiratory symptoms in the last 14 days on the HSQ, or a fever of 37.5 degrees or higher were investigated by the quarantine doctor.
(C) The personal care packages. Packages were distributed to each passenger it contained a personal hand sanitizer (50 mL), in-flight behavior guide, HSQ, a pen, and an extra face mask.
(D) A safety guide to the use of the toilet. A guide to safe use of the toilet was prepared and pasted on the mirror (blue dotted line). The guide is as follows. Use a disposable toilet seat cover. After using the toilet, close the toilet lid and flush. Open the toilet lid again and pump the diluted sodium hypochlorite into the toilet 3 or 4 times. A bottle of hand sanitizer (yellow solid line) and a bottle of 1:1,000 diluted sodium hypochlorite (red dotted line) were installed.
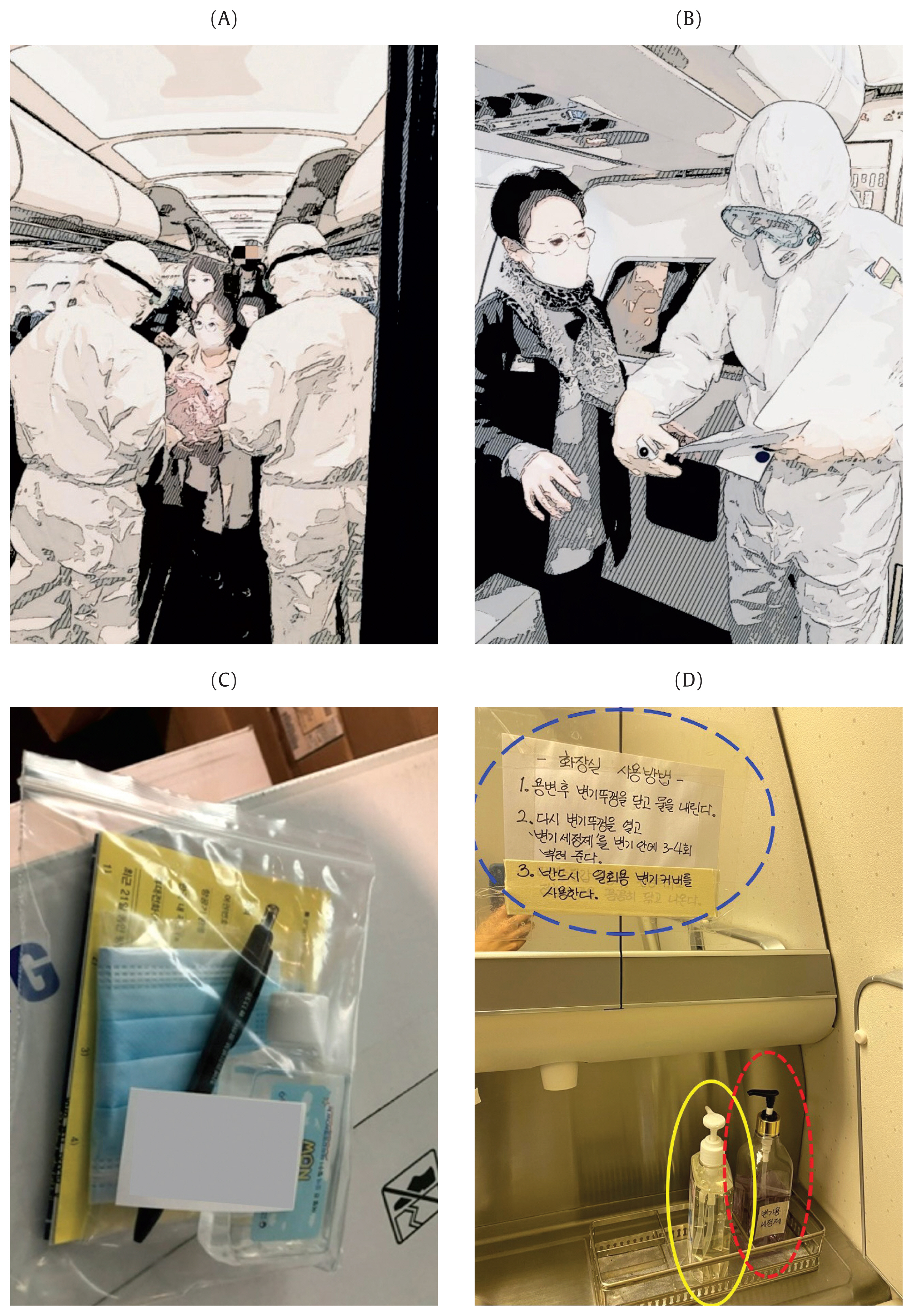
Figure & Data
References
Citations
Citations to this article as recorded by 
- International travel-related control measures to contain the COVID-19 pandemic: a rapid review
Jacob Burns, Ani Movsisyan, Jan M Stratil, Renke Lars Biallas, Michaela Coenen, Karl MF Emmert-Fees, Karin Geffert, Sabine Hoffmann, Olaf Horstick, Michael Laxy, Carmen Klinger, Suzie Kratzer, Tim Litwin, Susan Norris, Lisa M Pfadenhauer, Peter von Philip
Cochrane Database of Systematic Reviews.2021;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite