
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 14(4); 2023 > Article
-
Original Article
Mental health and its determinants among adolescents living in families with separated or divorced parents in an urban area of Vietnam -
Binh Thang Tran1
 , Minh Tu Nguyen2, Minh Tam Nguyen1,3, Thanh Gia Nguyen1, Vo Nu Hong Duc1, Thi Tra My Tran4
, Minh Tu Nguyen2, Minh Tam Nguyen1,3, Thanh Gia Nguyen1, Vo Nu Hong Duc1, Thi Tra My Tran4 -
Osong Public Health and Research Perspectives 2023;14(4):300-311.
DOI: https://doi.org/10.24171/j.phrp.2023.0110
Published online: August 9, 2023
1Faculty of Public Health, Hue University of Medicine and Pharmacy, Hue University, Hue, Vietnam
2Undergraduate Training Office, Hue University of Medicine and Pharmacy, Hue University, Hue, Vietnam
3Family Medicine Department, Hue University of Medicine and Pharmacy, Hue University, Hue, Vietnam
4Department of Psychiatry, Hue University of Medicine and Pharmacy, Hue University, Hue, Vietnam
- Corresponding author: Binh Thang Tran Faculty of Public Health, Hue University of Medicine and Pharmacy, Hue University, 06 Ngo Quyen Street, Hue City, Thua Thien Hue, Vietnam E-mail: tranbinhthang@hueuni.edu.vn
- Binh Thang Tran, Minh Tu Nguyen, and Minh Tam Nguyen equally contributed joins as the co-first authors.
© 2023 Korea Disease Control and Prevention Agency.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
- 2,211 Views
- 171 Download
Abstract
-
Objectives
- We assessed the prevalence of stress, anxiety, and depression among adolescents living in families with separated or divorced parents in Hue City, Vietnam and identified factors associated with these conditions.
-
Methods
- This cross-sectional study enrolled 309 adolescents, aged 12 to 17 years, living in families with separated or divorced parents in Hue City, Vietnam. The depression anxiety stress scale-21 (DASS-21) was used to measure stress, anxiety, and depression. Predictors of overall and individual mental health problems were identified using ordered and binary logistic regression, respectively.
-
Results
- The DASS-21 scale revealed a 49.2% prevalence of stress, while anxiety and depression had s prevalence rates of 61.5%. Among participants, 42.4% experienced all 3 mental health issues. Several factors were identified as significant predictors of mental health problems, including poor to average economic status (adjusted odds ratio [aOR], 2.00; 95% confidence interval [CI], 1.21–3.31; p=0.007); being in high school (aOR, 5.02; 95% CI, 2.93–8.60; p<0.001); maternal occupation of teacher, healthcare professional, or official (aOR, 2.39; 95% CI, 1.13–5.03; p=0.022); longer duration of family separation or divorce (aOR, 1.24; 95% CI, 1.05–1.45; p=0.009); living with one’s mother (aOR, 1.69; 95% CI, 1.03–2.76; p=0.04); alcohol consumption (aOR, 1.70; 95% CI, 0.99–2.92; p=0.050); and being bullied (aOR, 5.33; 95% CI, 1.10–25.69; p=0.037). Most of these factors were associated with stress, anxiety, and depression. Additionally, smoking was associated with stress.
-
Conclusion
- Adolescents with separated or divorced parents were at increased risk of stress, anxiety, and depression. The findings of this study provide important implications for prevention programs.
- Adolescence is a crucial period of physical, emotional, and social change that has a major impact on the health and well-being of young individuals. With 1.2 billion adolescents worldwide, adults and families must provide support and guidance as they navigate through life. Amidst numerous economic, cultural, and social shifts, adolescents encounter various health challenges, including mental health issues. The World Health Organization has reported that approximately 15% of children and adolescents experience mental health problems, making it the primary cause of disability for this age group [1].
- Vietnam contains approximately 14 million adolescents aged 10 to 19 years, with two-thirds residing in rural areas. Recent data from a United Nations Children’s Fund national survey revealed that approximately 8% to 29% of children and young people are at risk of mental health problems, with rates varying by province, gender, and respondent population and depending on the study measurement approach [2]. A 2022 study conducted in Hanoi, the largest urban area in northern Vietnam, found that 38% of middle school students experienced anxiety, 33% reported stress, and 26.1% exhibited depression [3]. Similarly, another recent study among high school students reported prevalence rates of stress, anxiety, and depression at 41.7%, 49.0%, and 43.6%, respectively, primarily at mild and moderate levels [4]. Consequently, mental health among students is a public health concern that necessitates attention and effective intervention from both family and school perspectives. The family and school environment play a significant role in adolescent development, and parental separation negatively impacts academic performance and mental health [5]. Stress, anxiety, and depression are common mental health disorders faced by children living with divorced parents, with girls being more vulnerable than boys [6]. The prevalence of mental health problems in this population can also be attributed to factors such as family structure, socioeconomic conditions, cultural background, and parents’ lack of knowledge about children’s health issues [6].
- Numerous studies have identified factors that contribute to an increased likelihood of stress, anxiety, and depression. A cross-sectional survey conducted among junior high school students in Malaysia and Greece revealed that parental marital status significantly increased the risk of depression, with participants from separated or divorced families facing 2 to 3 times higher risk than those with biological parents living together [7,8]. Similarly, a study conducted in Lebanon indicated a link between parental separation and adolescent anxiety [9]. Recent research conducted in Vietnam has also demonstrated that the quality of the parent-child relationship, grade level, and female gender are factors associated with depression, anxiety, and stress disorders among middle school students [3]. According to a previous study, children with divorced parents experience depression, anxiety, and thoughts of suicide at rates 1.29, 1.12, and 1.48 times higher, respectively, than children without divorced parents. They also have an increased likelihood of engaging in risky behaviors such as drinking alcohol (1.43 times) and smoking (1.64 times) [10].
- Vietnam, like other low-middle-income countries, has experienced rapid economic growth and urbanization in recent years. Such changes may also promote a shift in societal and family structures, particularly in people’s perceptions of parenting and marriage roles [11]. According to data from the 2019 Viet Nam General Statistics Office, the divorce rate has risen over the last decade, increasing from 1.11% in 2007 to 2.92% in 2017 among the population aged 15 years and older [12,13]. The divorce rate was found to be higher among women and those living in urban areas [11]. Several factors have been identified in the Vietnamese context to explain the high divorce rate, including lifestyle differences, adultery, domestic violence, social issues, and economic problems [12]. Additionally, as the age at first marriage increases, so does the divorce rate. This trend results in a greater number of adolescents living in divorced families [11].
- Numerous studies have recently investigated the prevalence of mental health issues; however, the findings in the general adolescent population may not accurately represent the situation for those living in families affected by separation or divorce. To our knowledge, this is the first study to be conducted on this subject. In terms of practical implications, the present research is anticipated to provide evidence for more effective interventions to address mental health issues in this population.
- Aims
- The aims of this study were to ascertain the prevalence of stress, anxiety, and depression among middle and high school adolescents with separated or divorced parents, utilizing the depression anxiety stress scale-21 (DASS-21) tool, and to pinpoint the factors influencing mental health among the study participants.
Introduction
- Participants and Study Design
- In October 2022, a cross-sectional study was conducted at 2 middle schools and 2 high schools in Hue City, Vietnam. A total of 342 students were invited to participate; however, 33 were excluded due to non-response or refusal by their guardians. Consequently, 309 eligible participants met the inclusion criteria, which included adolescent age, parental divorce/separation, and approval from both students and guardians.
- Minimal Sample Size Calculation
- In this study, we used the single proportion formula with a 95% confidence interval (CI) to calculate the sample size. This calculation was based on the previous prevalence rates of each DASS-21 subscale item among high school students in Hue City: 46.1% for stress, 68.2% for anxiety, and 49.6% for depression [14]. We aimed for a precision level of 6%, which resulted in a calculated sample size of 267. Considering a maximum non-response rate of 15%, the final calculated sample size was adjusted to 314 participants. Ultimately, we collected data from 309 of the 342 invited high school students who chose to participate in this study.
- Data Collection Process
- All students from separated or divorced families were invited to participate. We used convenience sampling to select 4 schools from a total of 26 public middle and high schools for inclusion in the study.
- The data collection for this study was carried out in several stages. Initially, a pilot survey was conducted among 20 high school students to assess the content and flow of the questionnaire. Subsequently, middle and high school teachers were enlisted to help identify potential participants. Data collectors were then trained in data collection techniques and addressing questions regarding the questionnaire. Students were provided with an information sheet and a consent form, which required the signature of their parents or guardians before participating in the survey. Once consent was obtained, students completed the survey using a self-administered questionnaire enclosed in an envelope. Upon completion, each student sealed the responses in the envelope and returned it to the collaborating teacher. The research supervisor then reviewed all questionnaires before submitting them to the principal investigator. In cases where students exhibited mild to severe symptoms, their teachers, parents, or guardians were notified, and the students were referred to free psychological counseling services.
- Variables and Measurement
- Three mental health problems—stress, anxiety, and depression—were measured using the DASS, specifically the DASS-21 scale, a well-known self-report form. This measurement tool has been well-validated and widely used in various populations in Vietnam, including adolescents [15]. The aim of the DASS-21 is to detect stress, anxiety, and depression in both clinical and non-clinical settings. The scale consists of 21 items, divided into 3 subscales of 7 items each: depression, anxiety, and stress. Respondents rated each item on a 4-point Likert scale, ranging from 0 (indicating that the item did not apply to them at all) to 3 (indicating that the item applied most of the time). The total score for each subscale was calculated by summing the scores of the 7 items, with a range of 0 to 21; higher scores indicated greater severity. For classification purposes, the suggested thresholds for each subscale were as follows [16]. For stress, scores of 0 to 14 were interpreted as normal, 15 to 18 as mild, 19 to 25 as moderate, and ≥26 as severe; participants with scores greater than 17 were considered to have stress. For anxiety, scores of 0 to 7 were considered normal, 8 to 9 mild, 10 to 14 moderate, and ≥15 severe; a score greater than 7 was interpreted as indicating anxiety. For depression, scores of 0–9 were interpreted as normal, 10 to 13 as mild, 14 to 20 as moderate, and ≥21 as severe; a score greater than 9 was considered to indicate having depression.
- In our analysis, we calculated the sum of all 3 DASS-21 subscales—stress, anxiety, and depression—to represent a spectrum of mental health issues and provide an overall measure of the mental health burden among respondents.
- Demographic information, including age, gender, birth order, and academic performance in the previous semester (average, good, or very good to excellent), as well as current living arrangements (living with mother or living with father), and school level (middle school [grades 6 to 9] or high school [grades 10 to 12]) was provided.
- Information on parental and family structure encompassed the education level (illiteracy/primary school, middle school, high school, or higher) and occupation (teacher/healthcare professional/official, housewife/worker/farmer, or business) of both mother and father, the household economic status (poor to average or normal), and the number of years since separation or divorce.
- Data on health-risk behaviors were also collected, including smoking (current smoking status), drinking (current drinking status), physical inactivity (measured by frequency and duration of activity per week, in accordance with World Health Organization recommendations), and engagement in fighting (frequency and involvement in physical altercations). Participants were also surveyed about their experiences of being bullied or physically assaulted. This questionnaire was recently used in the 2019 national survey among teenagers aged 13 to 17 years from the Global School-based Student Health Survey Vietnam [17].
- Data Analysis
- The primary data were entered and analyzed using Stata ver. 16.0 (StataCorp LP), with p-values less than 0.05 considered to indicate statistical significance. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were computed for all data. Due to significant differences in mental health problems between middle school and high school students, we stratified the results by school level when describing the prevalence of stress, anxiety, and depression. We combined all 3 DASS-21 subscales and classified them as ordinal categorical variables, with students grouped as follows: no mental health issues, only 1 issue, 2 of the 3 issues, and all 3 issues. Based on this outcome, we conducted a cumulative odds ordinal logistic regression with proportional odds to determine the relationship between factors and overall mental health problems. A multivariate binary logistic model was also employed to analyze the association between factors and individual subscales of the DASS-21. The Hosmer-Lemeshow test was utilized to evaluate the goodness of fit of the logistic regression model, enabling assessment regardless of the number and nature (quantitative or qualitative) of the independent variables.
- Ethical Consideration
- The study received ethical approval from the Institutional Ethics Committee for Biomedical Research at Hue University of Medicine and Pharmacy in Hue City, Vietnam (code: H2021/424, dated 26/8/2021). The principals of each school granted permission to conduct the study. Before completion of the questionnaires, parents/guardians were given information about the study and asked to provide written informed consent. Participants were informed of their right to voluntarily participate in the study.
Materials and Methods
Dependent variables
Independent variables
- Table 1 displays the general characteristics of the study participants. Among the 309 schoolchildren, 56.6% were male, with an equal distribution of students across the school levels. Two-thirds of the total sample size originated from households classified as poor to average in economic status. A large proportion of participants were either the eldest or the youngest child in their family, and two-thirds resided with their mothers. Furthermore, the majority of students’ parents had attained a high school education. The average duration of family separation or divorce was 3.02 years.
- Regarding health-risk behaviors, 11.0% of students reported smoking, 42.7% reported alcohol consumption, and 68.0% reported physical inactivity. A high prevalence of alcohol use was noted among high school students.
- Additionally, 8.7% of students reported involvement in fights, 8.1% indicated experiencing physical assault, and 5.5% reported being bullied. These rates were higher among middle school students.
- As shown in Table 2, the DASS-21 scale indicated a prevalence of 49.2% for stress, while both anxiety and depression had similar prevalence rates of 61.5%. Among those experiencing anxiety and depression, 29.1% and 19.7% reported severe to extremely severe levels, respectively. Additionally, high school students exhibited a higher prevalence of mental health issues compared to middle school students. Notably, the proportion of high school students classified as having very severe anxiety was quite high, at 24.4%. A detailed distribution of all items can be found in Table 3.
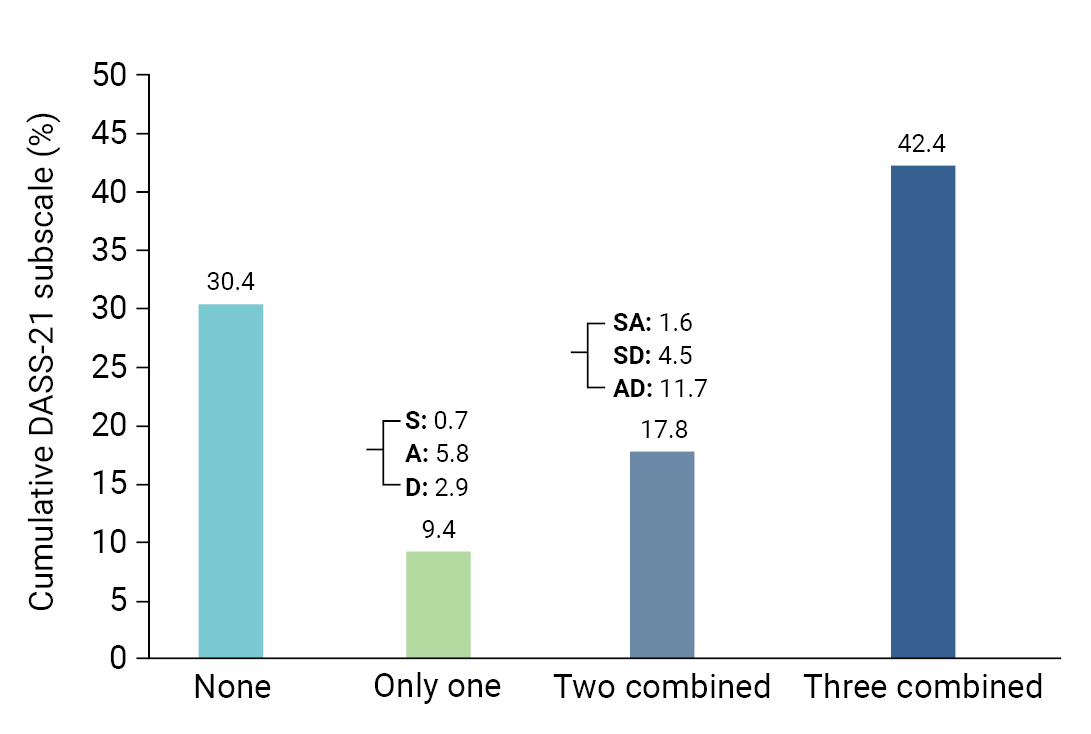
- Figure 1 depicts the prevalence of various mental health issues among the students. The survey revealed that 42.4% of the participating students experienced all 3 mental health problems, while 17.8% reported having 2 issues. Only 9.4% reported having a single mental health problem. Consequently, the overall percentage of students with mental health problems was 69.6%.
- Table 4 presents the results of an ordered logistic regression analysis examining factors associated with an increased risk of mental health problems in the study population. The analysis revealed several statistically significant predictors of various mental health problems, including poor to average economic status (adjusted odds ratio [aOR], 2.00; 95% CI, 1.21–3.31; p=0.007); being in high school (aOR, 5.02; 95% CI, 2.93–8.60; p<0.001); maternal occupation of teacher, healthcare professional, or official (aOR, 2.39; 95% CI, 1.13–5.03; p=0.022); longer duration of family separation or divorce (aOR, 1.24; 95% CI, 1.05–1.45; p=0.009); living with one’s mother (aOR, 1.69; 95% CI, 1.03–2.76; p=0.04); consuming alcohol (aOR, 1.70; 95% CI, 0.99–2.92; p=0.050); and being bullied (aOR, 5.33; 95% CI, 1.10–25.69; p=0.037).
- The results of multivariate binary logistic regression for each subscale revealed that predictors of stress included poor to average economic status (aOR, 1.97; 95% CI, 1.07–3.62; p=0.029); being in high school (aOR, 5.02; 95% CI, 2.74–9.18; p<0.001); maternal occupation of teacher, healthcare professional, or official (aOR, 4.06; 95% CI, 1.59–10.39; p=0.003); and current smoking (aOR, 3.15; 95% CI, 1.05–9.41; p=0.040). A marginal association was observed between being bullied (aOR, 6.21; 95% CI, 0.99–38.94; p=0.051) and experiencing stress.
- The results of multivariate binary logistic regression regarding the predictors of anxiety revealed several significantly associated factors: poor to average economic status (aOR, 2.05; 95% CI, 1.13–3.72; p=0.018); being in high school (aOR, 4.29; 95% CI, 2.31–7.97; p<0.01); maternal middle school education level (aOR, 3.09; 95% CI, 1.04–9.20; p=0.043); longer duration of family separation or divorce (aOR, 1.27; 95% CI, 1.06–1.53; p=0.011); and current alcohol consumption (aOR, 2.00; 95% CI, 1.04–3.84; p=0.037).
- Several factors were found to be significantly associated with depression, including poor to average economic status (aOR, 2.75; 95% CI, 1.47–5.17; p=0.002), being in high school (aOR, 6.28; 95% CI, 3.27–12.07; p<0.001); longer duration of family separation or divorce (aOR, 1.22; 95% CI, 1.01–1.48; p=0.041); living with one’s mother (aOR, 2.40; 95% CI, 1.20–4.42; p=0.005); current alcohol consumption (aOR, 2.73; 95% CI, 1.35–5.52; p=0.005); and being bullied (aOR, 20.12; 95% CI, 1.49–271.27; p=0.024).
- All 4 regression models underwent goodness-of-fit testing using the Hosmer-Lemeshow chi-square test. The p-values for all tests were determined to be greater than 0.05, indicating good fit for the models.
Results
- Summary of Findings
- This study was the first to investigate the prevalence of stress, anxiety, and depression among adolescents from separated or divorced families in Hue City, Vietnam and to identify associated factors. The results showed that 49.2%, 61.5%, and 61.5% of respondents reported experiencing stress, anxiety, and depression, respectively. Nearly half of the respondents reported negative emotional states across all 3 subscales (42.4%), while 7 in 10 reported encountering at least 1 of the 3 states. A high proportion of anxiety and depression cases were classified as severe or very severe. Several factors were found to be positively associated with an increased occurrence of mental health problems, including lower economic status; being a high school student; maternal occupation of teacher, healthcare professional, or official; longer duration of family separation or divorce; living with one’s mother; drinking alcohol; and being bullied. Lower economic status and being a high school student were found to have significant independent associations with all 3 DASS-21 subscales. Additionally, being subjected to bullying was independently associated with increased levels of both stress and depression. Furthermore, residing in a separated or divorced family for an extended period and current alcohol consumption were associated with a higher risk of experiencing depression and anxiety. Finally, having a mother employed as a teacher, healthcare professional, or official and current smoking were independently linked to elevated stress levels.
- Previous Findings Globally and in Vietnam
- Research on the effects of parental divorce/separation on adolescents has been relatively scarce in the public health literature. The authors endeavored to collect all relevant documents pertaining to this subject within the context of Vietnam, but we discovered only a small number of studies. In one past study, Son et al. [18] investigated prevalent psychological challenges and determined that children from non-intact families undergo psychological trauma. This trauma is evident in their emotions and attitudes towards both their family and their social lives.
- Our study is unique in that it is the first to examine mental health issues among this specific group. We compared the rates of depression, anxiety, and stress to those of the general population to identify any differences. A survey conducted among students aged 11 to 18 years (grades 6 to 11) found that approximately 26% reported a moderate to high risk of experiencing mental health issues [19]. Another study with a sample of 403 participants aged 12 to 17 years reported an overall rate of mental health problems of 33.1% [2]. When compared to similar instruments used to identify depression, anxiety, and stress among the general adolescent and high school populations, the DASS-21 subscale item rates were higher in our study (generally above 70% in high school and greater than 32% to 45% in middle school). For example, Huong et al. [14] reported rates of depression, anxiety, and stress (measured using the DASS-21) at 46.1%, 68.2%, and 49.6%, respectively, among high school students. Moreover, 32.7% of the students reported experiencing all 3 conditions (depression, anxiety, and stress). In 2 other studies in Hanoi among middle school students, the prevalence of depression (identified using DASS-21) was 27% [20], anxiety 38%, and stress 33% [3]. Studies conducted globally have demonstrated that divorce can significantly impact the mental health of adolescents, increasing their risk of developing symptoms of anxiety, depression, and stress. For instance, a study conducted in Lebanon found that 57.1% and 45.8% of adolescents from divorced families reported experiencing depression and social anxiety, respectively [21].
- The findings of this study are of utmost importance, as the high self-report rate serves as an alarming indicator of an underlying issue that demands urgent attention. Considering the high prevalence of mental health problems among adolescents with separated or divorced parents, early screening, diagnosis, and treatment should be integrated into routine health check-up programs. Furthermore, providing counseling support at school is an essential initial step, particularly since the understanding of students’ mental health, especially for those with separated or divorced parents, remains incomplete. Previous studies have identified adolescents as a particularly susceptible group to experiencing stressful events, such as parental divorce [22,23]. This vulnerability is attributed to the numerous physical, mental, emotional, and social changes that transpire during this developmental stage, which can influence future health patterns [24,25]. Our findings align with these previous studies.
- Factors Associated with Mental Health Problems
- The study findings revealed significant associations between multiple factors and both the cumulative scale and individual subscales of the DASS-21. These findings align with prior research that has identified similar risk factors for mental health issues among adolescents. However, the study results also emphasize the distinct characteristics of individuals whose parents are separated or divorced.
- In this study, we discovered that a longer duration of separation or divorce was associated with a 24% increased risk of mental health issues. This finding aligns with numerous longitudinal studies that have demonstrated significant increases in emotional and behavioral problems among adolescents following parental divorce, which persist over time [26,27]. These effects can be enduring and underscore the necessity of providing improved care for children of divorced parents [28].
- Several studies have indicated that children who experience parental divorce at an older age generally exhibit less severe issues relative to those who experience it at a younger age [29]. However, our research did not uncover any statistically significant relationship between child age and the prevalence of mental health problems. Furthermore, we observed a significant difference between middle school and high school students. This observation aligns with a study carried out by Ho et al. [30] in the same city, which suggests that life satisfaction significantly contributes to moderating the indirect impact of academic stress on depressive disorders, particularly among high school students.
- Our findings specifically indicate that children living with their mothers had a 1.69 times higher likelihood of experiencing mental health problems compared to those living with their fathers, a relationship that was particularly strong for depression (2.4 times higher). Although parental concern is often considered to reduce the risk of poor well-being in adolescents, excessive and overprotective maternal concerns due to increased risks, such as assault, suicidal ideation, and loneliness, have been strongly associated with mental health difficulties [31−33]. A longitudinal follow-up study in Norway discovered that the absence of a father figure in the family increased the risk of depression and anxiety, especially in boys [34]. However, our study did not investigate the level of attention provided by parents, which is a limitation.
- Moreover, this study revealed that students whose mothers possessed high stability and knowledge of labor occupations also experienced an increased risk of stress. This can be attributed to the Asian social context, in which high academic and societal expectations exist for children. This leads to heightened pressure in school and life, ultimately contributing to increased stress [19,35].
- The study results indicate that household economic status is a significant family factor associated with an increased risk of mental health issues, as indicated by both cumulative scores and each of the 3 individual subscales. This finding aligns with previous studies that emphasize family income as an important factor in this relationship [2,19,36]. It is widely acknowledged that low socioeconomic status during childhood negatively impacts psychological development and well-being [37]. Furthermore, economic issues within families may lead to separation or divorce, resulting in higher rates of these occurrences [11]. Providing social services to educate and support positive parenting practices in families facing economic challenges could be a valuable resilience strategy [38].
- The study identified early alcohol consumption as a major consequence of parental divorce, which contributes to an increased risk of mental health issues in children, particularly anxiety and depression [39,40]. Furthermore, bullying was strongly associated with a higher risk of depression, as demonstrated by studies in Vietnam [41−43]. Another study by Obeid et al. [21] discovered that adolescents with divorced parents were relatively likely to experience social fear and avoidance, depression, and suicidal ideation. These findings underscore the importance of school and community mental health intervention programs devoting greater attention to this vulnerable population and incorporating risk reduction strategies into their plans.
- The results of this study offer numerous suggestions for intervention and future research. Considering the high prevalence of stress, anxiety, and depression among adolescents from separated or divorced families, it is essential to provide mental health services to these young individuals.
- Future research can build upon the findings of the current study by examining the specific mechanisms through which family factors affect adolescent mental health outcomes. Longitudinal studies can aid in establishing causal relationships between these factors and mental health outcomes, while qualitative studies can offer a deeper understanding of the experiences of adolescents from separated or divorced families. Furthermore, future research can explore the influence of cultural factors on adolescent mental health outcomes in divorced families, as cultural norms and values may significantly impact the experiences of adolescents in this context.
- The current study had several limitations that should be considered when interpreting the results. First, the cross-sectional design of the study and the combined mental health outcome limited our ability to establish causal relationships between the variables of interest. Second, selection bias may have been present due to the exclusion of private schools from this study. Furthermore, the class teacher’s sample list was used to confirm the separation and divorce status of the minor’s parents, which somewhat restricted the definition, as it did not require specific certification. Finally, the use of a questionnaire may have introduced information bias due to potential difficulties in understanding the questions and overestimation or underestimation of symptoms, which could result in inaccuracies. Despite these limitations, the study had a notable strength in that it is the first to be conducted among this vulnerable group, providing a more detailed understanding that will support the future development of prevention and intervention strategies. Additionally, we received enthusiastic support from the class teachers, school principals, and even a student council president during the study.
Discussion
- The results of our study suggest that adolescents whose parents are separated or divorced have an increased risk of encountering mental health issues. This highlights the importance of implementing suitable prevention programs to assist them during this emotionally difficult period, particularly for those living with their mothers, experiencing low socioeconomic status, and participating in risky behaviors.
Conclusion
- • This is the first comprehensive survey examining the mental health of adolescents living in families with separated or divorced parents in urban Vietnam.
- • Nearly half of the surveyed adolescents reported experiencing negative emotional states, such as stress, anxiety, and depression, as measured by the depression anxiety stress scale-21.
- • The duration of family separation or divorce, low socioeconomic status, experience of bullying, and engagement in risky health behaviors were identified as significant predictors of poor mental health among the surveyed population.
HIGHLIGHTS
-
Ethics Approval
The study received ethical approval from the Institutional Ethics Committee for Biomedical Research at Hue University of Medicine and Pharmacy in Hue City, Vietnam (code: H2021/424, dated 26/8/2021). The principals of each school granted permission to conduct the study. Before completing the questionnaires, parents/guardians were given information about the study and asked to provide written informed consent. Participants were informed of their right to voluntarily participate in the study.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
The research was supported by funding from Hue University (DHH 2021-04-155).
-
Availability of Data
The datasets are not publicly available; however, they can be obtained from the corresponding author upon reasonable request.
-
Authors’ Contributions
Conceptualization: BTT, MTuN, MTaN; Data curation: MTuN, VNHD, TTMT, TGN; Formal analysis: BTT, MTuN, TGN; Funding acquisition: all authors; Methodology: BTT, MTaN; Project administration: VNHD, TTMT; Visualization: VNHD, TTMT, TGN; Writing–original draft: BTT, MTuN, MTaN; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Article information
| Factor |
Combinationa) |
Stressb) |
Anxietyb) |
Depressionb) |
||||
|---|---|---|---|---|---|---|---|---|
| aOR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Sex (ref: male) | ||||||||
| Female | 1.27 (0.78–2.07) | 0.332 | 1.59 (0.89–2.86) | 0.118 | 1.02 (0.58–1.80) | 0.935 | 1.25 (0.69–2.28) | 0.465 |
| Household economic status (ref: good) | ||||||||
| Poor to average | 2.00 (1.21–3.31)c) | 0.007c) | 1.97 (1.07–3.62)c) | 0.029c) | 2.05 (1.13–3.72)c) | 0.018c) | 2.75 (1.47–5.17)c) | 0.002c) |
| Academic school (ref: middle) | ||||||||
| High school | 5.02 (2.93–8.60)c) | <0.001c) | 5.02 (2.74–9.18)c) | <0.001c) | 4.29 (2.31–7.97)c) | <0.001c) | 6.28 (3.27–12.07)c) | <0.001c) |
| Academic performance (ref: good) | ||||||||
| Average | 1.10 (0.59–2.07) | 0.758 | 0.74 (0.34–1.59) | 0.439 | 0.98 (0.46–2.06) | 0.954 | 1.63 (0.74–3.57) | 0.222 |
| Very good to excellent | 0.73 (0.42–1.29) | 0.284 | 0.70 (0.36–1.36) | 0.297 | 0.76 (0.39–1.46) | 0.412 | 0.76 (0.38–1.53) | 0.446 |
| Mother’s education (ref: primary school or less) | ||||||||
| Middle school | 1.67 (0.7–4.01) | 0.251 | 1.11 (0.39–3.19) | 0.845 | 3.09 (1.04–9.20)c) | 0.043c) | 1.48 (0.49–4.48) | 0.491 |
| High school | 1.80 (0.78–4.16) | 0.168 | 1.49 (0.54–4.08) | 0.439 | 1.89 (0.70–5.12) | 0.212 | 1.63 (0.57–4.72) | 0.364 |
| Higher education | 0.80 (0.32–2.00) | 0.630 | 0.53 (0.17–1.65) | 0.275 | 1.28 (0.43–3.85) | 0.657 | 0.83 (0.26–2.70) | 0.763 |
| Mother’s occupation (ref: business) | ||||||||
| Housewife/worker/famer | 0.84 (0.48–1.47) | 0.540 | 0.94 (0.46–1.91) | 0.866 | 0.82 (0.42–1.61) | 0.560 | 0.81 (0.4–1.63) | 0.555 |
| Teacher/healthcare professional/official | 2.39 (1.13–5.03)c) | 0.022c) | 4.06 (1.59–10.39)c) | 0.003c) | 1.62 (0.69–3.81) | 0.266 | 1.96 (0.8–4.82) | 0.142 |
| Father’s education (ref: primary school or less) | ||||||||
| Middle school | 0.68 (0.28–1.62) | 0.382 | 0.79 (0.28–2.22) | 0.659 | 0.68 (0.24–1.91) | 0.467 | 0.64 (0.22–1.91) | 0.424 |
| High school | 0.46 (0.20–1.09) | 0.079 | 0.46 (0.17–1.30) | 0.144 | 0.60 (0.22–1.64) | 0.318 | 0.52 (0.18–1.52) | 0.232 |
| Higher education | 0.61 (0.24–1.55) | 0.299 | 0.58 (0.19–1.74) | 0.330 | 0.78 (0.26–2.29) | 0.650 | 0.73 (0.23–2.32) | 0.597 |
| Father’s occupation (ref: business) | ||||||||
| Housewife/worker/famer | 0.83 (0.45–1.53) | 0.544 | 0.85 (0.40–1.79) | 0.664 | 0.83 (0.40–1.73) | 0.620 | 0.80 (0.38–1.71) | 0.567 |
| Teacher/healthcare professional/official | 0.66 (0.29–1.48) | 0.312 | 0.51 (0.19–1.40) | 0.192 | 0.98 (0.38–2.56) | 0.974 | 0.71 (0.26–1.94) | 0.504 |
| Order of child in the family (ref: only child) | ||||||||
| Oldest | 1.32 (0.67–2.57) | 0.423 | 1.65 (0.75–3.62) | 0.216 | 1.38 (0.63–2.99) | 0.419 | 0.75 (0.33–1.72) | 0.503 |
| Middle | 1.33 (0.62–2.87) | 0.465 | 0.75 (0.30–1.91) | 0.548 | 2.38 (0.92–6.20) | 0.075 | 1.08 (0.41–2.88) | 0.876 |
| Youngest | 1.58 (0.81–3.08) | 0.178 | 1.54 (0.70–3.38) | 0.284 | 1.53 (0.71–3.30) | 0.277 | 0.93 (0.41–2.10) | 0.859 |
| Year of divorce | 1.24 (1.05–1.45)c) | 0.009c) | 1.10 (0.91–1.32) | 0.332 | 1.27 (1.06–1.53)c) | 0.011c) | 1.22 (1.01–1.48)c) | 0.041c) |
| Parent lived with (ref: father) | ||||||||
| Mother | 1.69 (1.03–2.76)c) | 0.04c) | 1.29 (0.72–2.32) | 0.394 | 1.35 (0.76–2.40) | 0.302 | 2.40 (1.20–4.42)c) | 0.005c) |
| Current smoking (ref: no) | ||||||||
| Yes | 2.03 (0.81–5.07) | 0.130 | 3.15 (1.05–9.41)c) | 0.040c) | 1.15 (0.4–3.26) | 0.796 | 1.27 (0.41–3.91) | 0.679 |
| Current drinking (ref: no) | ||||||||
| Yes | 1.7 (0.99–2.94)c) | 0.050c) | 1.48 (0.79–2.79) | 0.223 | 2.00 (1.04–3.84)c) | 0.037c) | 2.73 (1.35–5.52)c) | 0.005c) |
| Being beaten (ref: no) | ||||||||
| Yes | 0.93 (0.27–3.21) | 0.908 | 0.72 (0.17–3.12) | 0.660 | 1.92 (0.41–9.06) | 0.410 | 0.91 (0.18–4.57) | 0.908 |
| Being bullied (ref: no) | ||||||||
| Yes | 5.33 (1.1–25.69)c) | 0.037c) | 6.21 (0.99–38.94)c) | 0.051c) | 5.24 (0.67–40.78) | 0.114 | 20.12 (1.49–271.27)c) | 0.024c) |
| Fighting (ref: no) | ||||||||
| Yes | 1.63 (0.54–4.91) | 0.387 | 2.94 (0.82–10.55) | 0.098 | 0.73 (0.21–2.55) | 0.624 | 1.09 (0.28–4.19) | 0.900 |
| Physical inactivity (ref: no) | ||||||||
| Yes | 0.68 (0.39–1.16) | 0.154 | 0.56 (0.29–1.08) | 0.081 | 0.57 (0.30–1.10) | 0.094 | 0.66 (0.33–1.32) | 0.240 |
| /cut1 | 1.34 (−0.07 to 2.75) | |||||||
| /cut2 | 1.91 (0.49–3.32) | |||||||
| /cut3 | 2.89 (1.45–4.33) | |||||||
| Hosmer-Lemeshow χ2 | χ2=26.43, p=0.439, pR2=24.2% | χ2=6.41, p=0.600, pR2=24.3% | χ2= 5.04, p=0.754, pR2=19.5% | χ2=4.91, p=0.767, pR2=26.0% | ||||
- 1. World Health Organization (WHO). Adolescent health [Internet]. WHO; 2019 [cited 2023 Apr 1]. Available from: https://www.who.int/health-topics/adolescent-health.
- 2. UNICEF. Mental health and psychosocial wellbeing of children and young people in selected provinces and cities in Viet Nam. UNICEF Vietnam; 2014. Co-published by the Overseas Development Institute.
- 3. Vinh NA, Loan DM, Tu DH, Van PT. [Factors related to depression, anxiety and stress disorders in students in Tay Son and Nguyen Du Secondary School–Hanoi]. J Pediatr Res Pract 2022;6:1Vietnamese.
- 4. Nguyen DL, Le MG, Mai TP, Nguyen TD, Nguyen TT. Risk of stress, anxiety, depression of high school students Yen Dinh, Thanh Hoa. Vietnam Med J 2022;516:67−70. Vietnamese.
- 5. Theunissen MH, Klein Velderman M, Cloostermans AP, et al. Emotional and behavioural problems in young children with divorced parents. Eur J Public Health 2017;27:840−5.ArticlePubMed
- 6. D'Onofrio B, Emery R. Parental divorce or separation and children’s mental health. World Psychiatry 2019;18:100−1.ArticlePubMedPMCPDF
- 7. Magklara K, Bellos S, Niakas D, et al. Depression in late adolescence: a cross-sectional study in senior high schools in Greece. BMC Psychiatry 2015;15:199. ArticlePubMedPMCPDF
- 8. Ang AL, Wahab S, Abd Rahman FN, et al. Depressive symptoms in adolescents in Kuching, Malaysia: prevalence and associated factors. Pediatr Int 2019;61:404−10.ArticlePubMedPDF
- 9. Haddad C, Chidiac J, Sacre H, et al. Prevalence and associated factors of social anxiety among Lebanese adolescents. Prim Care Companion CNS Disord 2022;24:21m03061. ArticlePubMed
- 10. Auersperg F, Vlasak T, Ponocny I, et al. Long-term effects of parental divorce on mental health: a meta-analysis. J Psychiatr Res 2019;119:107−15.ArticlePubMed
- 11. Long TQ. Characteristics of marriage in Vietnam. J Fam Gend Stud 2021;31:73−81. Vietnamese.
- 12. Thi Minh Thi T. Complex transformation of divorce in Vietnam under the forces of modernization and individualism. Int J Asian Stud 2021;18:225−45.Article
- 13. General Statistics Office of Vietnam. Results of the 2019 Viet Nam population and housing census. General Statistics Office of Vietnam; 2020.
- 14. Huong NT, Diem DT, Duc VN, Thuy PT, Tri TT. Depression, anxiety, stress among high school students in Hue city, 2020-2021. Vietnam J Prev Med 2022;32:85−92. Vietnamese.
- 15. Le MT, Tran TD, Holton S, et al. Reliability, convergent validity and factor structure of the DASS-21 in a sample of Vietnamese adolescents. PLoS One 2017;12:e0180557.ArticlePubMedPMC
- 16. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther 1995;33:335−43.ArticlePubMed
- 17. World Health Organization (WHO). Report of the 2019 global school-based student health survey in Viet Nam. WHO; 2022.
- 18. Son HV, My NT, Vu GT, et al. The psychological trauma expressions of children living in the non-intergrity fammily through emotions and feelings regarding family and social life. Dalat Univ J Sci 2019;9:45−54. Vietnamese.
- 19. UNICEF. Comprehensive Study on school-related factors impacting mental health and well-being of adolescents in Viet Nam. UNICEF; 2022.
- 20. Nguyen DK, Le MT, Ngo AV. Risk of stress, anxiety, depression of high school students Yen Dinh, Thanh Hoa. Vietnam Med J 2023;526(1A). Vietnamese.
- 21. Obeid S, Al Karaki G, Haddad C, et al. Association between parental divorce and mental health outcomes among Lebanese adolescents: results of a national study. BMC Pediatr 2021;21:455. ArticlePubMedPMCPDF
- 22. Low NC, Dugas E, O'Loughlin E, et al. Common stressful life events and difficulties are associated with mental health symptoms and substance use in young adolescents. BMC Psychiatry 2012;12:116. ArticlePubMedPMCPDF
- 23. Chase-Lansdale PL, Cherlin AJ, Kiernan KE. The long-term effects of parental divorce on the mental health of young adults: a developmental perspective. Child Dev 1995;66:1614−34.ArticlePubMed
- 24. Moretti MM, Peled M. Adolescent-parent attachment: bonds that support healthy development. Paediatr Child Health 2004;9:551−5.ArticlePubMedPMC
- 25. Sawyer SM, Afifi RA, Bearinger LH, et al. Adolescence: a foundation for future health. Lancet 2012;379:1630−40.ArticlePubMed
- 26. Tullius JM, De Kroon ML, Almansa J, et al. Adolescents’ mental health problems increase after parental divorce, not before, and persist until adulthood: a longitudinal TRAILS study. Eur Child Adolesc Psychiatry 2022;31:969−78.ArticlePubMedPDF
- 27. O'Hara KL, Sandler IN, Wolchik SA, et al. Parenting time, parenting quality, interparental conflict, and mental health problems of children in high-conflict divorce. J Fam Psychol 2019;33:690−703.ArticlePubMedPMC
- 28. Ba Nguyen D, Van Nguyen L. Mental health among left-behind children in Vietnam: role of resilience. Int J Ment Health 2022 Jul 12 [Epub]. https://doi.org/10.1080/00207411.2022.2098562.
- 29. Zeratsion H, Dalsklev M, Bjertness E, et al. Parental divorce in late adolescence does not seem to increase mental health problems: a population study from Norway. BMC Public Health 2013;13:413. ArticlePubMedPMCPDF
- 30. Ho TT, Nguyen BT, Nguyen NP. Academic stress and depression among Vietnamese adolescents: a moderated mediation model of life satisfaction and resilience. Curr Psychol 2022;1−11.ArticlePDF
- 31. Nguyen HT, Nakamura K, Seino K, et al. Impact of parent-adolescent bonding on school bullying and mental health in Vietnamese cultural setting: evidence from the global school-based health survey. BMC Psychol 2019;7:16. ArticlePubMedPMCPDF
- 32. La TT, Dinh HT, Phan MT, et al. Mental health among Vietnamese urban late adolescents: the association of parenting styles. Health Psychol Open 2020;7:2055102920948738. ArticlePubMedPMCPDF
- 33. Coles DC, Cage J. Mothers and their children: an exploration of the relationship between maternal mental health and child well-being. Matern Child Health J 2022;26:1015−21.ArticlePubMedPDF
- 34. Storksen I, Roysamb E, Moum T, et al. Adolescents with a childhood experience of parental divorce: a longitudinal study of mental health and adjustment. J Adolesc 2005;28:725−39.ArticlePubMedPDF
- 35. Van TP. The relationship between parents’ expectations and mental health of high school students in Ho Chi Minh City, Viet Nam. Int J Mod Trends Soc Sci 2021;4:19−27.Article
- 36. Sands A, Thompson EJ, Gaysina D. Long-term influences of parental divorce on offspring affective disorders: a systematic review and meta-analysis. J Affect Disord 2017;218:105−14.ArticlePubMed
- 37. Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med 2013;90:24−31.ArticlePubMed
- 38. Lee MC, Huang N, Chen CY. Effects of childhood adversity trajectories on mental health outcomes in late adolescence: the buffering role of parenting practices in Taiwan. Child Abuse Negl 2020;109:104705. ArticlePubMed
- 39. Richards M, Hardy R, Wadsworth M. The effects of divorce and separation on mental health in a national UK birth cohort. Psychol Med 1997;27:1121−8.ArticlePubMed
- 40. Kim EG. Multilevel analysis of the risk factors in high-risk health behavior among Korean adolescents. Osong Public Health Res Perspect 2018;9:3−8.ArticlePubMedPMCPDF
- 41. Le HT, Tran N, Campbell MA, et al. Mental health problems both precede and follow bullying among adolescents and the effects differ by gender: a cross-lagged panel analysis of school-based longitudinal data in Vietnam. Int J Ment Health Syst 2019;13:35. ArticlePubMedPMCPDF
- 42. Trong Dam VA, Do HN, Thi Vu TB, et al. Associations between parent-child relationship, self-esteem, and resilience with life satisfaction and mental wellbeing of adolescents. Front Public Health 2023;11:1012337. ArticlePubMedPMC
- 43. Phan TC, Chau B, Do HN, et al. Determinants of mental health among youths and adolescents in the digital era: roles of cyber and traditional bullying, violence, loneliness, and environment factors. Front Public Health 2022;10:971487. ArticlePubMedPMC
 Cite
Cite

