
Articles
- Page Path
- HOME > Osong Public Health Res Perspect > Volume 4(3); 2013 > Article
-
Original Article
Study on Entomological Surveillance and its Significance during a Dengue Outbreak in the District of Tirunelveli in Tamil Nadu, India - Parasuraman Baskera, Pichai Kannanb, Rajagopal Thirugnanasambandam Porkaipandiana,b, Sivsankaran Saravanana,b, Subramaniam Sridharana,b, Mahaligam Kadhiresana,b
-
Osong Public Health and Research Perspectives 2013;4(3):152-158.
DOI: https://doi.org/10.1016/j.phrp.2013.04.005
Published online: April 30, 2013
aZonal Entomological Team, Department of Public Health and Preventive Medicine, Tamil Nadu, India
bDirectorate of Public Health and Preventive Medicine, Tamil Nadu, India
- ∗Corresponding author. drbasker@yahoo.co.in
© 2013 Published by Elsevier B.V. on behalf of Korea Centers for Disease Control and Prevention.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives
- To study the significance of entomological surveillance, the house index (HI), container index (CI), and Breteau index (BI) were determined to estimate the degree of a major dengue outbreak in Tirunelveli, Tamil Nadu, India (Latitude: 8°42′N; Longitude: 77°42′E) in May 2012.
-
Methods
- The HI, CI, and BI were determined in a primary health center (PHC) in the village of Maruthamputhur (Pappakudi taluk, Tirunelveli) by carrying out an antilarval (AL) work that involved door-to-door search for immature stages of Aedes spp. mosquitoes by trained field workers and volunteers. The work of field workers was evaluated by a junior and senior entomologist the following day.
-
Results
- Before the AL work, the reported numbers of fever cases from Week 1 to 5 in Maruthamputhur were 211, 394, 244, 222, and 144 with two deaths. By contrast, after the AL work, these numbers were considerably reduced and there was no fever-related death (the HI was reduced from 48.2% to 1.6%, the CI from 28.6% to 0.4%, and the BI from 48.2 to 1.6).
-
Conclusion
- Because no specific medicine and vaccines are available to treat dengue fever and dengue hemorrhagic fever, entomological surveillance and its significance can be used to halt the outbreak of dengue as shown in this study.
- Dengue is an acute febrile illness caused by Flavivirus, which exists in four different serotypes, namely, DEN-1, DEN-2, DEN-3, and DEN-4. Its transmission is effected through female Aedes aegypti and Aedes albopictus mosquitoes (vectors). Dengue fever (DF) may transform into dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) and these conditions are fatal causing hemorrhages and leakage of plasma, respectively [1]. This mosquito-borne disease not only causes high levels of morbidity and mortality, but also has a great economic impact, including loss in commercial and labor output, particularly, in tropical and subtropical countries. However, no part of the world is free from these diseases [2]. To prevent and control the spread of dengue, various approaches have been attempted and most of them yielded fruitful results, with vector control proving to be the best approach until dengue-specific drugs and vaccines are developed [3]. There are three major components of dengue surveillance, namely, disease surveillance, vector surveillance, and monitoring of environmental and social risks. Among these components, entomological surveillance is used to determine changes in the geographical distribution and density of the vector, evaluate control programs, obtain relative measurements of the vector population over time, and facilitate appropriate and timely decisions regarding interventions [4]. A number of methods are available for detecting or monitoring immature and adult populations. Selection of appropriate sampling methods depends on the surveillance objectives, levels of infestation, available funding, and skills of personnel [5]. The objectives of A. aegypti surveillance methods are baseline infestation survey, control program monitoring low infestation levels [<5% house index (HI)], control program monitoring with ≥5% HI level, surveillance against reinfestation, verification of eradication, and evaluation of control methods. These objectives have been accomplished with larval survey, collecting data on mosquito landing on humans or biting them, collection of resting mosquitoes, ovitrap, tire larvitraps, and insecticide susceptibility based on their suitability [6].
- Several indices have been used to monitor A. aegypti populations for dengue virus transmission. Those related to immature populations are the HI, i.e., the percentage of house infested with larvae or pupae; the container index (CI), i.e., the percentage of water-holding containers infested with larvae or pupae; and Breteau index (BI), i.e., the number of positive containers per 100 houses inspected. When using the HI or the BI, the definition of a house should be one unit of accommodation and the surrounding premises, irrespective of the number of people residing therein [7,8].
- In this study, efforts have been made to understand the significance of entomological surveillance using the HI, CI, and BI during a dengue outbreak (May 2012) in Tirunelveli district of Tamil Nadu, India, and to incorporate the study findings in the dengue-control measure protocols.
Introduction
- 2.1 Active fever surveillance
- Information on fever was collected with the resources available by active (door-to-door search) and passive surveillance (institutional surveillance), as fever is the prime sign and symptom for DF. A door-to-door search (active surveillance) was performed by field staffs, health inspectors, and village health nurses during their field visits. Based on the data collected, malaria form 2 was filled in and a blood smear test was conducted to rule out malarial fever. The form along with the test results were sent to the medical officer at the primary health center (PHC). In addition, the S form of the Integrated Disease Surveillance Project (IDSP) was also filled out in order to understand the clinical syndromes of diseases such as malaria, dengue, leptospirosis, and acute diarrheal diseases in the community, with the case definition defined in the IDSP Manual [9]. A copy of the S form was also sent to the medical officer at the PHC. It would also be helpful to identify (using event-based surveillance) whether disease clusters are present in a place. Based on the reports submitted and laboratory test results, decisions can be made for implementing specific disease-control measures.
- 2.2 Case definition of dengue
- According to the IDSP manual, dengue is defined as an acute febrile illness of 2–7-day duration with two or more of the following symptoms: head ache, retro-orbital pain, myalgia, arthralgia, rash, hemorrhagic manifestations, and leucopenia.
- 2.3 Passive surveillance
- Passive surveillance is an institutional surveillance using which information about the spectrum of diseases can be obtained. For the present study, passive surveillance was used to collect daily information on fever from the outpatients of the PHCs and inpatients of government hospitals, private nursing homes, and sentinel surveillance hospitals (tertiary care hospitals such as medical college hospitals) in the district. Based on this information, the entomological surveillance was prioritized.
- 2.4 Entomological surveillance
- Entomological surveillance was used for the antilarval (AL) and antiadult measures. The AL work was performed by skilled field workers and trained volunteers by identifying immature stages of Aedes spp. in common mosquito habitats near the premises of human dwellings such as tires, coconut shells, cement cisterns, overhead tanks. These sources were removed with all possible efforts and in cases where removal was not possible larvicide [50% temephos (Abate) emulsified concentration at the dosage of 1 ppm] was used to kill the mosquito larvae.
- To manage manpower, the AL work was performed in a village by dividing it into six-day blocks from Monday to Saturday. All dwellings of each block were thoroughly checked by workers on the specified day. One worker was allotted for every 60 houses, so that sufficient numbers of workers are available to cover all the houses in a village. The 6-day block was recommended based on the life cycle of mosquitoes as it usually takes between 7 and 10 days for the imagoes to emerge from the eggs.
- Antiadult measures were carried out using ultralow-volume thermal fogging with a formulation of pyrethrum (a synthetic pyrethroid compound) and diesel in the ratio of 1:19. The fog was created by PulsFOG machines and vehicle-mounted fogging machines. Because dengue vectors A. aegypti and A. albopictus have diurnal periodicity, fogging was performed from 8 am to 11 am and from 3 pm to 5 pm following the condition of wind velocity and speed of vehicle (6–10 km/h). People were instructed to properly cover the food, keep the infants away from mosquito dwellings, keep the doors and windows open during fogging and close them after fogging for half an hour so as to ensure the knockdown effect of the insecticide [10].
- 2.5 Entomological indices
- Entomological indices, namely, HI, CI, and BI were computed from the daily data collected in the AL work for assessing its impact. To calculate these indices, the following formulae were used:
- Antiadult measures were assessed by bioassays and per man-hour density (PMHD) of mosquitoes through hand collection. The PMHD is number of mosquitoes collected by a man in an hour using a mechanical aspirator.
- 2.6 Appraising method for the AL work
- To appraise the AL work performed by the field staff and trained volunteers, a junior and senior entomologist investigated a minimum of 25 houses in which the field workers carried out the AL work the previous day. The data collected by the entomologists and field workers were matched and any inconsistency was discussed in the daily review meeting in order to improve the quality of work by the field workers. This method was continued every day until the outbreak was halted completely.
- 2.7 Community participation
- To encourage the communities to take part in vector-control measures, various information education and communication activities were conducted during the course of dengue outbreak, which included demonstration of Aedes larvae to the people in their house premises, information about the variety of habitats, periodicity of the mosquito as it is diurnal, importance of source reduction, and scrubbing of water-stored vessels as its eggs can withstand humidity for even a year and can resume life when the container becomes wet with water, the importance of weekly interventions of these activities as the life cycle of mosquitoes is only 7–10 days, etc. These activities were conducted in school meetings in which the students took oath during their daily prayers to control dengue by reducing the various sources of Aedes, antidengue awareness program through public addressing system, local telecast, and interpersonal communication.
- 2.8 Statistical analysis
- The values of the indices calculated by both field workers and appraisers were analyzed by Chi-square test using the Statistical Package of Social Sciences version 12.0 (SPSS Inc., Chicago, IL, USA). A p value < 0.05 was taken to be significant.
Materials and Methods
- This study was carried out in Maruthamputhur village (Tirunelveli, Tamil Nadu, India; Latitude 8°42′N, longitude 77°42′E) wherein there was a dengue outbreak in May 2012. The primary information on fever was obtained from various resources (Figure 1) to understand the degree of outbreak and to prioritize the AL and antiadult measures to be undertaken.
- To determine the impact of the entomological surveillance, the data collected on fever in a week were taken as before and after entomological intervention. Before the AL work, the reported numbers of fever cases from Week 1 to 5 in Maruthamputhur were 211, 394, 244, 222, and 144 with two deaths, which shows the magnitude of the problem. Among outpatients at PHCs in Maruthamputhur, all probable cases of dengue were identified according to the case definition in the IDSP manual. In accordance with this, nine, 36, 15, 10, and nine cases of fever (with an onset period less than 7 days) in Weeks 1–5, respectively, were referred to the sentinel hospital for laboratory confirmation. The test results were found to be positive for dengue virus infection based on the detection of NS1 antigen and immunoglobulin M (IgM) antibodies in IgM capture enzyme-linked immunosorbent assay (Figure 2).
- An observation on entomological surveillance data revealed that the HI, CI, and BI were above the permissible level in the 1st week of intervention, but their values gradually reduced after the AL and antiadult measures. The HI, CI, and BI was 48.2%, 28.6%, and 48.2% before the entomological intervention; however, after the intervention these indices were considerably reduced as the HI values were 10.2%, 5.2%, 2.5%, and 1.6% in the 2nd, 3rd, 4th, and 5th week, respectively; the CI values were 2.3%, 0.9%, 0.4%, and 0.3%, respectively; and BI values were 12.9%, 6.2%, 2.8%, and 1.6%, respectively. The weekly progress of Aedes indices during the entomological surveillance is shown in Figure 3. These findings reflected the considerable reduction in the population of Aedes spp. (both pupae and adult) and subsequently a reduction in the number of dengue cases reported. No deaths due to dengue were reported after the intervention (Figure 4).
- The AL work performed by field workers was appraised by a junior and senior entomologist who inspected a minimum of 25 houses. We also found that there was a consistent reduction in the value of the indices from the 1st week of intervention onward. When the data of appraisers were matched with those collected by field workers, some inconsistencies were found (p > 0.005). Because these data reflect the quality of AL work, inconsistencies were reviewed in the daily meetings in order to improve the quality of AL work. Among the referred cases, no death was reported from the 3rd week. The incubation period of the dengue virus is 4–14 days [11], which was also considered to appraise the quality of AL work, i.e., if the interventions were successful, there should be a descending trend from the second fortnight of intervention. In this study, cases in the first fortnight were 45, but it was reduced to 15, 9, and 0 in the subsequent fortnights, showing the success of the intervention.
- During the course of the outbreak, the following have also been observed and highlighted: the HI not only provides information about the geographical distribution, but it also useful as an evaluating tool. We ascertained how long dengue cases might have been prevailing in the community. Children (1–14 years) are more susceptible in the first phase (15 days from the onset of confirmed cases). Deaths indicated the existence of multiple serovars. Shifting of dengue-confirmed cases from children to adults (>14 years) indicated that the mortality rates would be less, as adults have better immunity than children. Any delays in the control of dengue cases within 15 days might reflect on the quality of AL work. While trying to stop the outbreak, the minimum permissible value for both HI and BI was 1.6%, considering the environmental condition of the village (Figure 5).
Results
- Entomological surveillance is an appropriate tool for the prevention and control of dengue outbreak until suitable vaccine and specific drugs for DF, DHF, and DSS are made available. It was ascertained by the World Health Organization (WHO) that preventing or reducing the transmission of dengue virus entirely depends on the control of the mosquito vectors or interrupting the human–vector contact [12,13]. The WHO ascertained that integrated vector management is the best strategic approach to control vectors in all vector-borne diseases, including dengue. The population of dengue vectors was greatly reduced by reducing their sources such as small containers in the premises of human dwellings [14]. It is a proven fact that dengue control is possible only through advocacy, social mobilization and legislation, collaboration within the health sector and other sectors, integrated approach to disease control, evidence-based decision making, and capacity building. Based on these approaches, a nonchemical control was suggested rather than a chemical control, because there is an increased resistance among mosquitoes for chemical controls, while its alternative, various plant alkaloids have also been tried in various dengue vector–control studies [2,15–18]. Above all, promoting the source reduction of Aedes species through the AL work along with community participation yielded good results and control of A. aegypti was mainly achieved by eliminating water-filled containers that are favorable oviposition sites, which permit the development of the aquatic stages. The habitats are eliminated by preventing access to these containers or by frequently emptying and cleaning them. In unavoidable situations, insecticides, biological control agents, or a combination of both were used, which kills the adult mosquitoes [19].
- Based on the references studied, there were concrete evidences to support the results of the present study in which an outbreak of dengue was effectively controlled through entomological surveillance by carrying out AL work and antiadult measures in the district of Tirunelveli in Tamil Nadu, India, rather than relying on chemical control to which mosquitoes have now become resistance as well as the difficulty in using such controls in clean water sources. By collecting daily reports of fever cases from PHCs, it is possible to know those places or villages that are most vulnerable. These villages could then be prioritized for implementing control measures. The importance of using Aedes indices has been proven as an effective tool as there was a rapid reduction in the number of dengue cases and mortality after the AL work. For monitoring the entomological surveillance, an appraising mechanism was used, which is also a novel method or a milestone to evaluate day-to-day control activities of dengue and to assess the quality of AL work. To improve the quality of the AL work, the incubation period of dengue (4–14 days) was considered during the appraising phase. These observations have the merits to be incorporated as a modus operandi in the prevention and control of dengue in any corner of the world.
Discussion
-
Acknowledgements
- The authors thank the field staffs who engaged in the AL work that was undertaken during the dengue outbreak in Tirunelveli (Tamil Nadu, India) in May 2012. We are especially thankful to the Mr Vijaykumar (Junior Entomologist, Filaria and Malaria Clinic, Tamil Nadu) and Mr Dhanasekaran (Laboratory Technician of the Zonal Entomological Team) for their real involvement in evaluating the AL work to assess its quality. Besides, we are also grateful to the Deputy Directors of Health Services and Senior Entomologist, Zonal Entomological Team, Tirunelveli for their guidance.
Acknowledgments
-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article information
- 1. World Health Organization . Dengue hemorrhagic fever: diagnosis, treatment, prevention and control. 1997. WHO; Geneva: p 84.
- 2. Fradin M.S., Day J.F.. Comparative efficacy of insect repellents against mosquito bites. N Engl J Med 347(1). 2002 Jul;13−18. PMID: 12097535.ArticlePubMed
- 3. World Health Organization . Dengue: guidelines for diagnosis, treatment, prevention and control. 2009. WHO; Geneva: p 146.
- 4. Basker P., Ezhil R.. Study on the correlation of premises condition index and the presence of larvae of Aedes species mosquitoes in human dwellings of the Cuddalore district of Tamil Nadu, India. Osong Public Health Res Perspect 3(1). 2012 Mar;3−7.ArticlePubMed
- 5. World Health Organization . Dengue and dengue hemorrhagic fever. 2002. WHO; Geneva: p 117.
- 6. Pan American Health Organization (PAHO) . Dengue and dengue hemorrhagic fever in the Americas: guidelines for prevention and control. 1994. PAHO; Washington.
- 7. Tun-Lin W., Kay B.H., Barnes A.. The premise condition index: a tool for streamlining surveys of Aedes aegypti. Am J Trop Med Hyg 53(6). 1995 Dec;591−594. PMID: 8561259.ArticlePubMed
- 8. Directorate General of Health Services, Government of India . Integrated Disease Surveillance Project (IDSP) training manual for state and district surveillance officers. 2005. Directorate General of Health Services; New Delhi: p 270.
- 9. World Health Organization . Equipment for vector control. 3rd ed.1990. WHO; Geneva: p 310.
- 10. Focks D.A., Chadee D.D.. Pupal survey: an epidemiologically significant surveillance method for Aedes aegypti: an example using data from Trinidad. Am J Trop Med Hyg 56(2). 1997 Feb;159−167. PMID: 9080874.ArticlePubMed
- 11. Gubler D.J.. Aedes aegypti and Aedes aegypti-borne disease control in the 1990s: top down or bottom up. Am J Trop Med Hyg 40(6). 1989 Jun;571−578. PMID: 2472746.ArticlePubMed
- 12. World Health Organization . Diagnosis, prevention and control. 2nd ed.1998. Prentice Hall India; New Delhi: pp 48−59.
- 13. Seng C.M., Jute N.. Breeding of Aedes aegypti (L.) and Aedes albopictus (Skuse) in urban housing of Sibu town, Sarawak. Southeast Asian J Trop Med Public Health 25(3). 1994 Sep;543−548. PMID: 7777923.PubMed
- 14. Kroeger A., Lenhart A., Ochoa M.. Effective control of dengue vectors with curtains and water container covers treated with insecticide in Mexico and Venezuela: cluster randomised trials. BMJ 332(7552). 2006 May 27;1247−1252. PMID: 16735334.Article
- 15. Mehlhorn H., Schmahl G., Schmidt J.. Extract of the seeds of the plant Vitex agnus-castus proven to be highly efficacious as a repellent against ticks, fleas, mosquitoes and biting flies. Parasitol Res 95(5). 2005 Mar;363−365. PMID: 15682335.ArticlePubMed
- 16. Cetin H., Erler F., Yanikogu A.. Larvicidal activity of a botanical natural product, AkseBio2, against Culex pipiens. Fitoterapia 75(7–8). 2004 Dec;724−728. PMID: 15567250.ArticlePubMed
- 17. Govindarajan M.. Larvicidal and repellent activities of Sida acuta Burm. F. (Family: Malvaceae) against three important vector mosquitoes. Asian Pac J Trop Med 3(9). 2010 Sep;691−695.Article
- 18. Govindarajan M., Karupannan . Mosquito larvicidal and ovicidal properties of Eclipta alba (L.) Hassk (Asteraceae) against chikungunya vector, Aedes aegypti (Linn.) (Diptera: Culicidae). Asian Pac J Trop Med 4(1). 2011 Jan;24−28. PMID: 21771410.ArticlePubMed
- 19. World Health Organization . Global strategic framework for integrated vector management. 2004. WHO; Geneva.
References
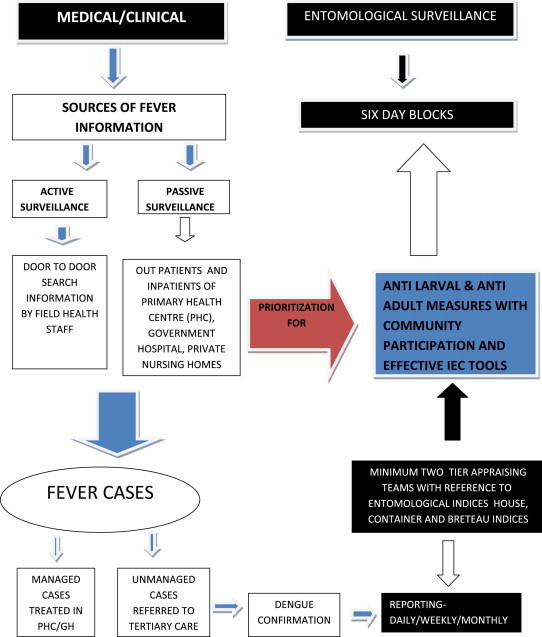

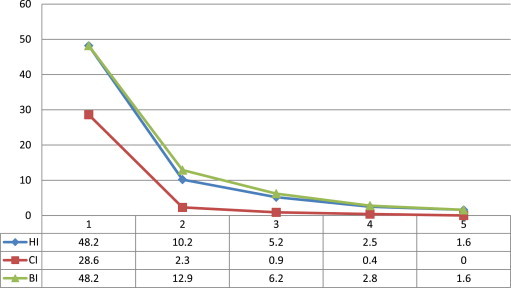

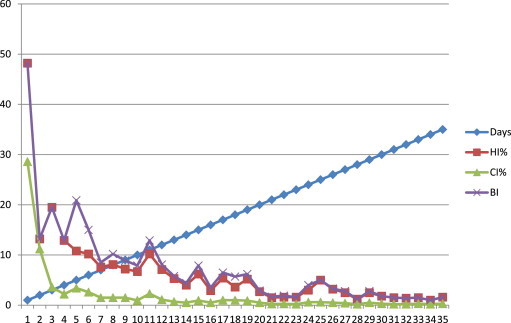
Figure & Data
References
Citations
- Morphological and molecular characterization of Aedes aegypti variant collected from Tamil Nadu, India
PNirmal Kumar, M Kalimuthu, MSenthil Kumar, R Govindrajan, A Venkatesh, R Paramasivan, Ashwani Kumar, Bhavna Gupta
Journal of Vector Borne Diseases.2022; 59(1): 22. CrossRef - Larval survey and spatial epidemiological analysis of vector Aedes aegypti to study the risk of dengue outbreak in India
A. Sajeli Begum, Swati Alok, Samrun Nessa
GeoJournal.2021; 86(1): 81. CrossRef - Estimating the annual dengue force of infection from the age of reporting primary infections across urban centres in endemic countries
Joseph R. Biggs, Ava Kristy Sy, Katharine Sherratt, Oliver J. Brady, Adam J. Kucharski, Sebastian Funk, Mary Anne Joy Reyes, Mary Ann Quinones, William Jones-Warner, Ferchito L. Avelino, Nemia L. Sucaldito, Amado O. Tandoc, Eva Cutiongco-de la Paz, Maria
BMC Medicine.2021;[Epub] CrossRef - Comparison of INAR(1)-Poisson model and Markov prediction model in forecasting the number of DHF patients in west java Indonesia
Atina Ahdika, Novyan Lusiyana
Journal of Physics: Conference Series.2017; 814: 012002. CrossRef - Identification of Aedes albopictus
larval index thresholds in the transmission of dengue in Guangzhou, China
Lei Luo, Xiaoning Li, Xincai Xiao, Ya Xu, Miaoling Huang, Zhicong Yang
Journal of Vector Ecology.2015; 40(2): 240. CrossRef
 PubReader
PubReader Cite
Cite




